
If you want to work 1-on-1 with me, DM me "ENERGY", and we'll see what we can do! Any doubts on my content, or anything that I can help you with, just lmk 👍
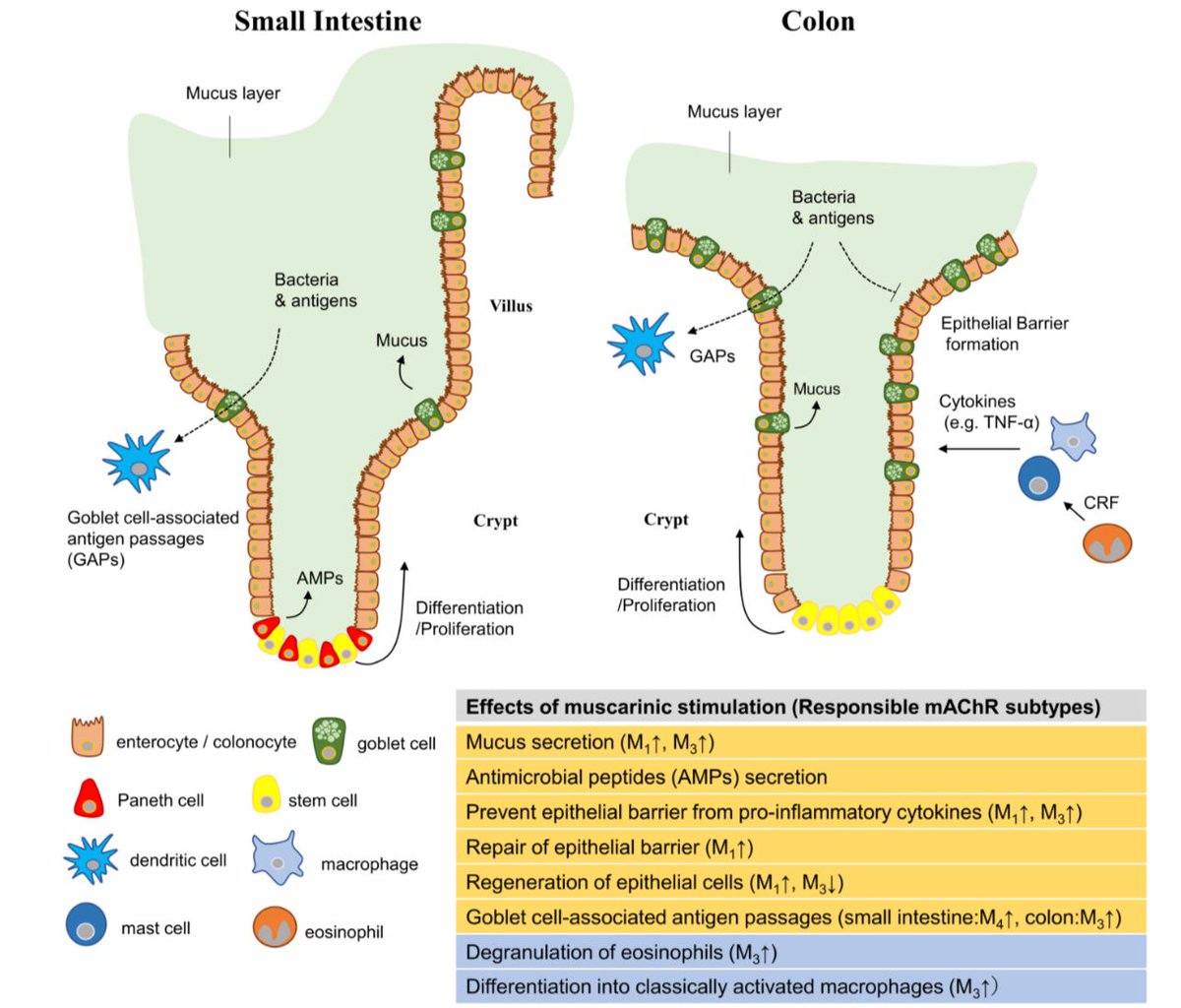
 Unlike the large intestine, the small intestine is NOT meant to harbor a microbiome.
Unlike the large intestine, the small intestine is NOT meant to harbor a microbiome.



 • Electrolytes & Magnesium 🌊
• Electrolytes & Magnesium 🌊




 CONCLUSION
CONCLUSION  More like immunostimulant power but you get the idea 💯💯💯
More like immunostimulant power but you get the idea 💯💯💯
 Probiotic & micronutrient gets even moar based if it’s homemade Kefir 🥂
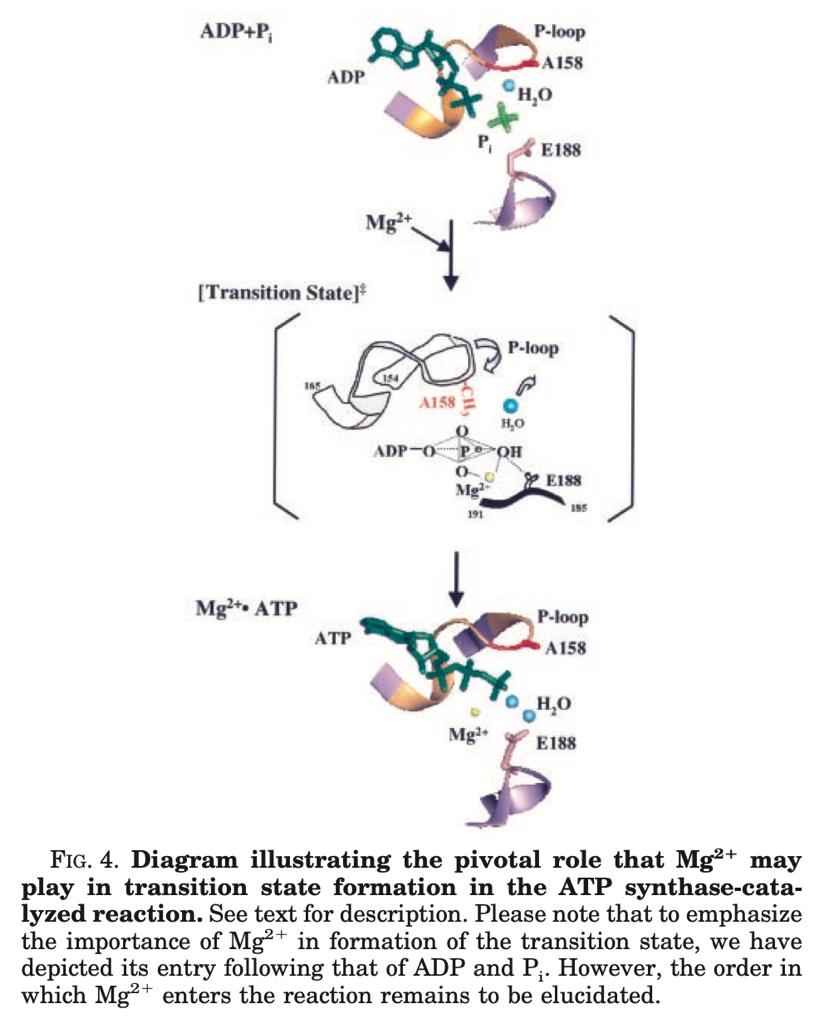
Probiotic & micronutrient gets even moar based if it’s homemade Kefir 🥂 Elongation = RNA “getting longer”, thanks to the addition of new nucleotides. Essentially the process of replication fr no cap
Elongation = RNA “getting longer”, thanks to the addition of new nucleotides. Essentially the process of replication fr no cap
 They even got negative results in their glucose homeostasis & insulin sensitivity!
They even got negative results in their glucose homeostasis & insulin sensitivity!

 If damaged, the “stomach cells” are exposed to HCL acid which leads to ulcers.
If damaged, the “stomach cells” are exposed to HCL acid which leads to ulcers. 


 JUST by drinking kefir for 2 months, all the 30 diabetics in the Kefir Group experienced a 30% improvement in their HOMA-IR! From 7.05 to 4.93!
JUST by drinking kefir for 2 months, all the 30 diabetics in the Kefir Group experienced a 30% improvement in their HOMA-IR! From 7.05 to 4.93!
 It’s literally delayed for the duration of a half time of a football match, or a whole workout (for lotta people). Unfair advantage.
It’s literally delayed for the duration of a half time of a football match, or a whole workout (for lotta people). Unfair advantage.
 Redefining the functional roles of the gastrointestinal migrating motor complex and motilin in small bacterial overgrowth and hunger signaling
Redefining the functional roles of the gastrointestinal migrating motor complex and motilin in small bacterial overgrowth and hunger signaling In fact, the cortex is just as metabolically active during the wake state - which requires high ACh activity as shown below, hence the name “Paradoxical Sleep” for REM sleep 👍👍👍👍
In fact, the cortex is just as metabolically active during the wake state - which requires high ACh activity as shown below, hence the name “Paradoxical Sleep” for REM sleep 👍👍👍👍 

 It is CRITICAL that during & after an injury (either physical or biochemical), viral infection or medication treatment you focus on getting enough Vitamin B1 and Magnesium
It is CRITICAL that during & after an injury (either physical or biochemical), viral infection or medication treatment you focus on getting enough Vitamin B1 and Magnesium
 Alright putos, so if you're dealing with:
Alright putos, so if you're dealing with: When I was broke and still had to go train football, me and my homie would still find ways to feed ourselves, and every training day I would wake up and think “tf we will eat today after training”
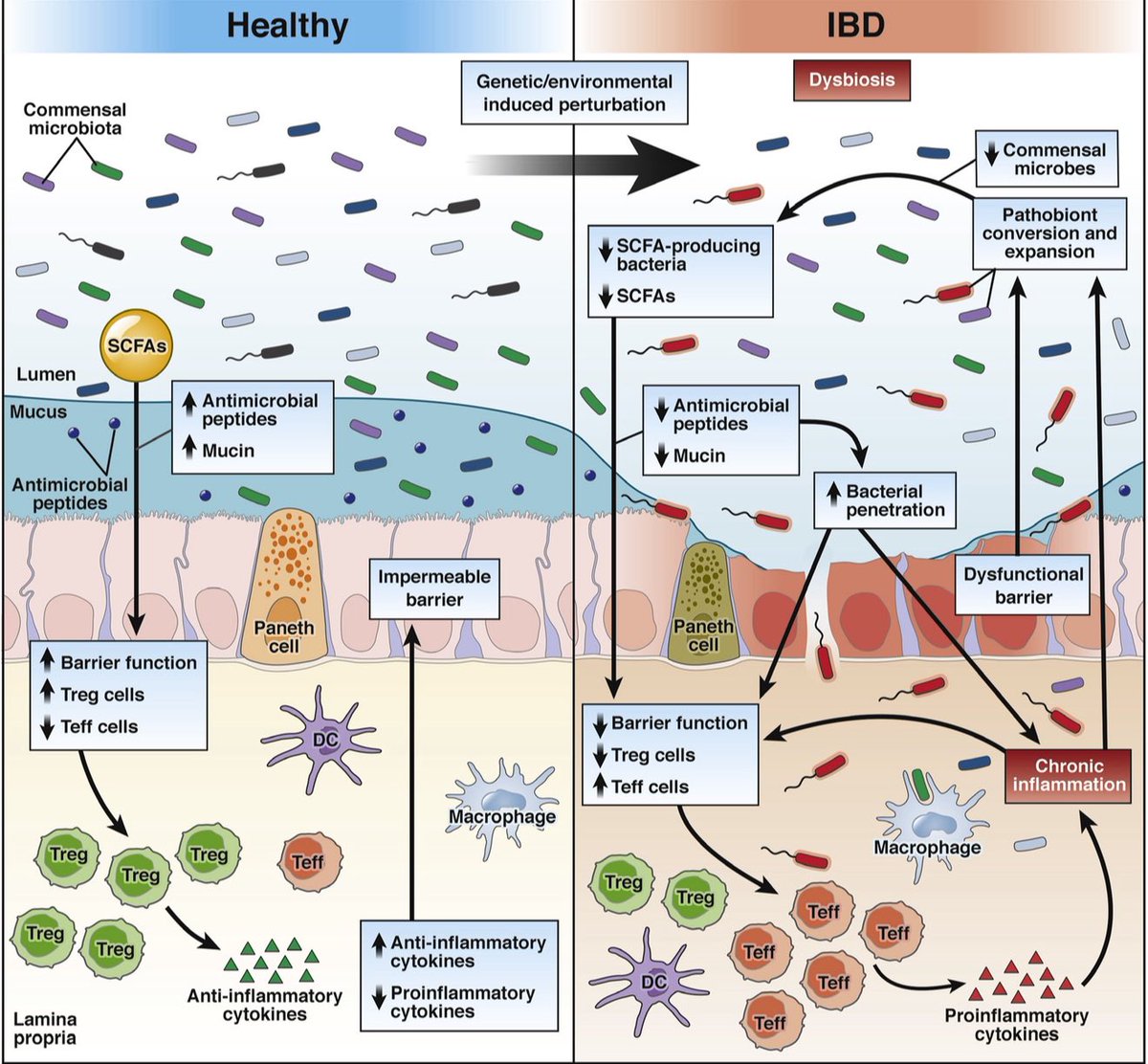
When I was broke and still had to go train football, me and my homie would still find ways to feed ourselves, and every training day I would wake up and think “tf we will eat today after training” And even though Butyrate is the least SCFA produced?
And even though Butyrate is the least SCFA produced? Literally just a ginger supplement had such effect - now imagine the effects whole fresh ginger root consumption would have had.
Literally just a ginger supplement had such effect - now imagine the effects whole fresh ginger root consumption would have had.