Health Economist and Associate Professor @Yale @YaleSPH @YaleEconomics @YaleTobinCenter @nberpubs
Dec 2, 2024 • 9 tweets • 3 min read
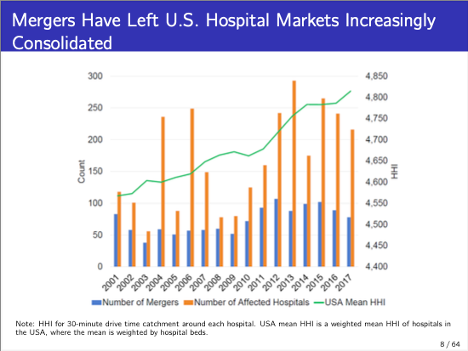
My new paper - Is There Too Little Antitrust Enforcement in the US Hospital Sector? - with @zarekcb @stuartcraig & @LevKlarnet was just published in AER: Impact (@AEAjournals). A Thread
From 2002 to 2020, there were over 1,000 hospital mergers and the US. During that period, the @ftc only took action against 13 🏥 deals. Our paper asks if the @FTC has historically done enough.
Jun 23, 2024 • 7 tweets • 3 min read
🚨🚨🚨🚨🚨 New Paper Alert 🚨🚨🚨🚨
A new paper with @zarekcb @stuartcraig @LevKlarnet, Ithai Lurie, and Corbin Miller analyzing the economic consequences of rising health spending. Amazing coverage from @melaevans and co. @wsj
TLDR Summary: Employer-sponsored health insurance creates a link between what happens in health care markets and what happens in labor markets. We show that when hospitals merge and prices go up, low- and middle-class workers lose their job. Along with job losses, we see a loss in tax revenue collected by the federal government.
Apr 24, 2024 • 15 tweets • 5 min read
🚨 New paper alert! “Is There Too Little Antitrust Enforcement in the US Hospital Sector?” with @zarekcb, @stuartcraig, and Lev Klarnet that’s forthcoming in American Economic Review: Insights. TLDR: Yes…there has been way too little enforcement. 🧵
Joint work with @JonSkinner17, Staiger, Ndumele, and Stiegman. We compare regional spending on Medicare, Medicaid (!), and the privately insured.
Do distinct factors drive spending variation by payer? (thread)
jamanetwork.com/journals/jaman…
We were focused on studying regional variation in spending across the three main funders of health care - Medicare, Medicaid, and the privately insured. This is important because nobody has really analyzed variation in Medicaid spending.
Jul 1, 2022 • 14 tweets • 7 min read
I'm a huge proponent of integrating the best academic evidence into journalism to inform reporting. In case useful, here's a tour of the academic evidence showing why price transparency likely won't do much. Hope this is useful for your reporting and reporting of others.
Often, this academic work is hard to access & written opaquely. There's an intuitive appeal of price transparency, but unfortunately, the evidence (and theory) doesn't suggest we should be optimistic. Hopefully, this thread helps highlight what research says on these issues
Jul 1, 2022 • 14 tweets • 7 min read
Today, insurers will be required, via a sensible Executive Order from President Trump, to post the prices they pay to providers. @Julie_appleby has a great story in @KHNews and @NPR. A brief thread on what the EO is going to do (hint, I don't think much). khn.org/news/article/h…
The data requirement for insurers will force payors to post the prices they pay for each item with each provider. This is actually the data I use for most of my research. In the past, this data was kept locked away and regarded as a 'trade secret'.
Feb 28, 2022 • 22 tweets • 10 min read
🚨New Paper Alert🚨
“Do Higher-Priced Hospitals Deliver Higher-Quality Care?” Joint w/Joe Doyle, @johngraves9, and Jon Gruber.
A thread with
- some surprising results re prices & quality
- evidence competition --> efficiency
- Policy recs
nber.org/papers/w29809
TLDR – summary: Receiving care from high-priced hospitals in concentrated markets ⬆️ spending by 52% but does not lead to lower mortality. Receiving care from high-priced hospitals in competitive markets ⬆️ spending by 52% and lowers mortality by 1.37 percentage points (~47%)!
Apr 8, 2021 • 20 tweets • 5 min read
Why is health spending in the US high?
This terrific episode of Freakonomics is focused on End Stage Renal Disease (ESRD). The issue is a window into why we spend a lot on health care in the US and the dysfunction in the system.
ESRD is on the rise in the US. In part, this is driven by the rise in diabetes in the US, which leads to ESRD. So, poor health management --> downstream problems.
A patient with ESRD can be 'cured' with a kidney transplant. While waiting for a transplant, they need dialysis.
Feb 10, 2021 • 16 tweets • 9 min read
🚨How do you reduce health spending?🚨
We are launching a new project - ‘1% Steps for Health Care Reform’. We're working with leading health policy scholars and the goal is harness research to illustrate tangible steps to reduce health care spending.
The core idea-if the US health system was a country, it’d be the 4th largest country in the world. There’s not 1 thing wrong in a system so big. There are lots of little problems that add up. We asked experts to identify discrete problems & propose reforms healthaffairs.org/do/10.1377/hbl…
Feb 10, 2021 • 18 tweets • 6 min read
🚨New Paper Alert (actually, old paper that just got published, but hey)🚨
@Michael_Chernew@ProfFionasm Columbia PhD student Eugene Larsen-Hallock and I examine whether health care is 'shoppable' by looking at how patients consume lower-limb MRI scans. sciencedirect.com/science/articl…
This dovetails nicely with paper out by @amitabhchandra2 and @oziadias earlier this week. Predictions from price theory are that if you ratchet up cost-sharing and give patients transparency tools, they'll consume health care services they way they consume peppers.
Dec 12, 2020 • 13 tweets • 4 min read
Big news on surprise billing .
There's a bicameral agreement on addressing surprise billing.
Overall, this isn't what I would have done, but arbitration linked to in-network payments isn't crazy.
The bipartisan proposal includes a hold harmless provision that requires patients, if treated by an out-of-network doctor at an in-network facility, only be subject to in-network cost-sharing & no balance billing (eg MDs/staffing companies can't go after them for charges). 2/n
Jul 10, 2020 • 10 tweets • 3 min read
New @politico op-ed by @stevenberry + me. We argue that Congress is grossly underfunding efforts to combat Covid-19 & that White House's wish it away strategy won't work. We need humility - we don't know what will work, so we should fund redundant programs politico.com/news/agenda/20…
Less than 8 percent of the trillions in funding that Congress has allocated so far in response to the virus has been for solutions that would shorten or mitigate the virus itself: increasing the supply of PPE, expanding testing, developing treatments, vaccine development.
Jun 12, 2020 • 4 tweets • 2 min read
.@ACEPNow pro ports to represent ED physicians. They trade on the good will of hardworking physicians but seem to be really benefitting EmCare and TeamHealth. In fact, as reporting by @sangerkatz@ReedAbelson and others show, they are actually working with the PE firms on comms
See this great piece in the @UpshotNYT that identified the PE firms and ED physician staffing companies behind the tsunami of political ads on surprise billing. nytimes.com/2019/09/13/ups…
Apr 12, 2020 • 13 tweets • 5 min read
🚨 To better advise some policy-makers we’re speaking with, what do we view as the key barriers to scaling up testing and strategies to overcome them. See thread below. Figured public sourcing would be helpful here. @ScottGottliebMD@paulmromer@steventberry@erikbryn
The returns to testing are MASSIVE. @ATabarrok has written about this. This is @Austan_Goolsbee first rule of virus Econ. If we assume daily costs of shutdown are in $billions, we should be spending huge amounts (100s of billions) to speed reopening marginalrevolution.com/marginalrevolu…
Feb 8, 2020 • 11 tweets • 2 min read
A big day of surprise billing proposals from the Hill yesterday. Below is a thread on the different options proposed by ED and Labor and Ways and Means, the trade-offs between arbitration and benchmarking, and possible ways to reconcile the ED+Labor and the Ways and Means plans
The Ways&Means plan includes a hold harmless proposal + arbitration where the arbitration is linked to in-network payments and there’s no cap on size of bills that go to arb.
ED & Labor has a hold harmless and uses benchmarks for bills < $750 and arbitration for bills > $750
Dec 21, 2018 • 12 tweets • 3 min read
Pump the brakes. In work with a vastly stronger empirical design, Atul Gupta found the program reduced mortality and readmissions. Observational studies have a role, but we can’t simply interpret them as causal. dropbox.com/s/rfwok9en2c58…@amitabhchandra2@asacarny
The Gupta study is really good. Below is a summary and some thoughts. He notes that hospitals could respond to readmissions penalties in two ways: 1) by improving quality or 2) by changing composition of patients they admit (e.g. not admitting patients