
Here are some rules I emphasize when teaching central line placement, usually for IJ triple lumens and HD lines. Not a comprehensive guide, just some things I've seen trainees miss (including myself). I'm a fellow so I am by no means an expert and I'd love your input! [THREAD] 

Prep is everything. Room, bed, trash, table, etc. Make it easy! Move bed up, IVs and trash on opposite side of table--make space. Raise bed. Head down. Confirm ultrasound(US), image the length of vessel (for overt clots/stenoses). Clean hair, leads, tubes out of the way.

Before starting, I ask everyone to alert me if I've broken sterility to create a global expectation. Breaking sterility happens, you didn't "mess up." Don't hesitate, just get more PPE. I always bring a few sets -- proper setup helps maintain sterility. Just ask my daughter!

Warn the pt before every stick. Even if sedated. Talk to them like they're awake and participating. Reassure them. They are incredibly vulnerable and you are doing something that could be quite anxiety provoking and could cause significant complications.
Use lidocaine, even if sedated. I've done plenty of lines in awake pts in the cath lab, sometimes w/o any IV meds- just plenty of lido! Beyond the wheal, try to inject deep, until tenting the vessel (but not in it!). You don't know what they can or can't feel, so just do it.

Angles & anatomy are critical. Can't compensate w US! My early lines were hard bc of poor position/angle. Chance of success, ability to track needle dramatically improved by initial angle & point of access.
If carotid is near, angle such that if you go deep you'll pass over it.
If carotid is near, angle such that if you go deep you'll pass over it.

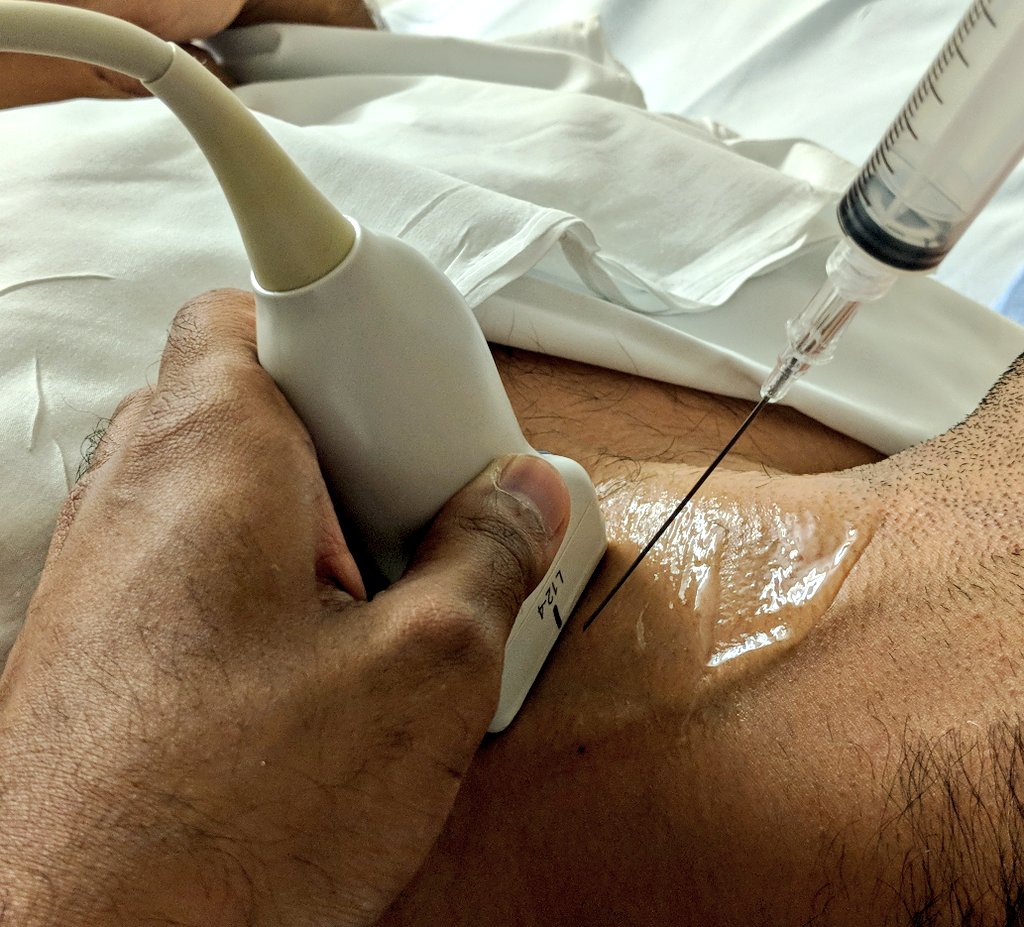
Stabilize the US with your hand on the patient. US should be rock steady--like a rhino! I hold it w two fingers as seen below. Use very fine motions to move along the vessel to find your needle tip- much slower and subtler than you think. Don't give up on this, you can find it!

If the wire isn't feeding, it isn't in the vessel. You should probably abandon and, importantly, flush your syringe/needle before trying again. Clots are common and can block the wire from passing. Once the wire is in, it should move smoothly in the vessel.
Never let go of the wire! So many people let go as they feed dilator/catheter into the pt. There is plenty of wire in the patient. Hold the catheter still, feed the wire back through it, don't attempt to advance it until you can grab the wire through the port.
If you do enough lines, you'll eventually puncture a carotid. It's ok, remove needle & hold pressure. NOT ok to dilate the carotid! To avoid, always US the wire in 2 planes. Look for target sign in axial & see wire come down into vessel in long axis, clearly avoiding carotid.

Use scalpel to nick the skin so dilator can pass, preparing for the catheter. I hold blade flat against wire & insert smoothly into skin. Depth depends on US image. The mistake here is to create a 'skin tag' between your nick & wire, which can be remedied with another nick.
Don't force dilator at an angle against skin, it can kink the wire. Advance to skin, hold dilator at the tip near the skin & twist in, through skin. If you are meeting too much resistance, you need to retract the dilator and make another nick, ensuring you don't have a skin tag.
Once the line is in, always draw back to get a flash in your syringe before flushing. By doing so you clear the line of air. Of course, don't flush the air back in!
Central lines are not easy, especially because they are less commonly used these days - many patients don't need central access. As a resident I'd go months between lines. Don't expect that you "should" be independent. Don't be over-confident. Ask for supervision!

I'd love to hear your thoughts and suggestions. Teaching procedures is incredibly rewarding and I'm always looking for ways to improve! #pulmcc
As noted by others some of the demos did not include appropriate PPE. To be clear, ALL central lines should be performed under sterile technique. The importance of this cannot be overstated. Thanks to our fantastic nurses for helping us maintain a sterile field!

• • •
Missing some Tweet in this thread? You can try to
force a refresh




