So. Hi new people! Apparently, we're gonna talk about sex. Like physical sex! Because... there's some confusion.
First, sex defined: We're talking physical sex here, not gender. Body parts, hormones, and genetics (and more).
BLUF: BIOLOGICAL sex is a spectrum
1/
First, sex defined: We're talking physical sex here, not gender. Body parts, hormones, and genetics (and more).
BLUF: BIOLOGICAL sex is a spectrum
1/
Ok, everyone's super familiar with the XX/XY dichotomy, right? Yeah, what we all learned in like... 4th grade? And that's great, it gives you a starting point. But it's... well it's only the very starting point.
The IDEA is, XX is girl, XY is boy, right?
2/
The IDEA is, XX is girl, XY is boy, right?
2/
Welllll... that's not totally right. There are XY people, who have ovaries! And give birth! AH! And XX people who have male bodies and functional sperm! Double AH!
3/
3/
These are usually written off as "abnormalities" and indeed, some cases have medical issues. But many don't (like the XY woman giving birth). And this is really only the very very tip of the iceberg of "wait, that doesn't fit into our M or F box unless we make it bigger"
4/
4/
There's a WHOLE HOST of things that can cause all sorts of "weird" things to happen, ranging from genetic (XXY, XYY, Y, X, XX with translocation, XY with deletion) to hormonal (Androgen Insensitivity, Estradiol failure), and disruptors like dioxins
/5
/5
So, you're a scientist, and you want to research stuff, right? Which means you have to categorize stuff. Without categories, data is hard! So you take allll these people, including the "weird" ones and you plot them on a graph. Logical!
/6
/6
You use all the differences there are, different genetics, different responses to hormones, different effectiveness in signalling pathways, different sizes in Aanteroventral periventricular nucleus (AVPV) (yeah that's a thing) and give everything numbers, add them up.
/7
/7
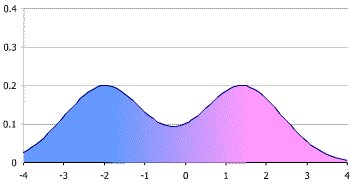
You get what's called a bimodal distribution (mostly, we'll get to that later) Which looks like this. Those two big peaks are what we call "male" and "female" (even conveniently colored pink for boys and blue for girls - we are using victorian gender colors right?)
/8
/8
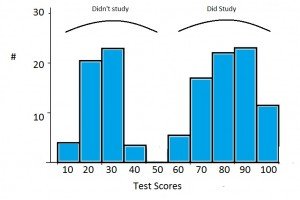
Now, when you're trying to look at data, we often group stuff. When we do that with a plot like this, it's called a "histogram." Basically we're breaking down a curved line into discrete "bins." Like this (image stolen from the web).
/9
/9
Traditionally, we've used REALLY BIG bins for this when talking about sex. Basically you either group everything vaguely near a peak into the peak, or you just pretend there's nothing else but the biggest peaks. This makes it super easy, because 2 is simple to do data with.
/10
/10
However, as we've gotten to know more and more about signaling and brains and hormones and started to pay more attention to the outliers where standard stuff just didn't seem to work, we discovered that this isn't a great model to use.
/11
/11
Now I'm not talking feelings here. I'm talking about data. As you start to look at anything interesting, like say the effects of 2,3,7,8-Tetrachlorodibenzo-P-dioxin on animals, you start to realize that a 2 bin model doesn't predict your results well.
/12
/12
At first you say, "Well it was just weird." So you redo it, and it still doesn't work. So you look at your model and you say, "Well ok, what if the model's wrong?"
But the model sort of... almost predicts a lot of things, and it worked for years, so...
/13
But the model sort of... almost predicts a lot of things, and it worked for years, so...
/13
Some enterprising soul says, "Hey, remember that histogram where we said we'll just model using the peaks?" And everyone goes, "Uh, yeah?" And they say, "What if we... USED that data?" And everyone groans, because complicated data is hard.
/14
/14
But someone sits down and does the work, and lo, wow the model starts to work again. Where TCDD was "randomly" turning some boys into girls but then some girls into boys, now you can see there's a subgroup of what you'd called "female" that responds like the "male"
/15
/15
What's important here is that you haven't MISLABELED males as females. These are functional "females" who can do all the usual "female" things like gestate babies. But they respond to this one endocrine disruptor in a "male" way.
/16
/16
So you add another two categories, call them "Male2" and "Female2" and go on, happy that your model works! You've got 4 sexes now, but you don't really have to tell anyone that, right?
/17
/17
Exceeeept then you remember you've got those XY people that gestate babies. So you add "Intersex1" And then the XX people with penes... and ovaries? Ok, "Intersex2" because all these groups respond differently with signalling and brains when you get into the weeds
/18
/18
And the more you look, the more we LEARN, the more we're able to separate out those fine differences. Depending on what we're doing, we may not care. If a doc is giving you aspirin, it probably isn't a big deal.
/19
/19
But if they're using a steroid on you? Or treating dioxin poisoning? THAT SHIT COULD BE IMPORTANT. It's like saying, "the light's off so the power must not be flowing." It really matters if the light's off because the bulb blew.
/20
/20
If we go back to that histogram plot, we can keep breaking down your biological sex into smaller and smaller differences in brain areas, hormone levels, signalling differences, genetic variances. There's nothing stopping us from binning EVERY INDIVIDUAL into their own bin.
/21
/21
Technically, this wouldn't be "infinite sexes" but 7.4 billion sexes is functionally close for our brains. Now, our medicine isn't advanced enough for THAT level of detail to make any difference. BUT IT MIGHT BE in the future. Individualized medicine!
/22
/22
The thing to remember is that this isn't "new." We're not 'inventing sexes' here. Sex has ALWAYS been this curve. We were just using REALLY BIG bins. And now we're realizing that that's not representative of biology, it's inhibiting understanding of medicine and biology
/23
/23
In case anyone's curious, this isn't ideology. This is because I had to figure out why my data didn't match the prediction. Those rats I mentioned? Yeah, my lab. And lab rats are a really pure genetic monoculture, and they STILL don't fit the two peak model well.
/24
/24
So, since it's come up, an addendum!
Yes, we looked at other things we could do to make our data fit the existing model, that's how science works! The ONLY way the data fit was if we let "sex" be more than just those two narrow peaks.
/25
Yes, we looked at other things we could do to make our data fit the existing model, that's how science works! The ONLY way the data fit was if we let "sex" be more than just those two narrow peaks.
/25
Models purpose in science is to predict. If they don't predict correctly, first we check if we've measured the data correctly, and repeat the experiment a couple more times. If it still doesn't fit, we have to look at the model.
/26
/26
Intersex! Because I didn't specifically mention this.
"Intersex" is a grouping bin used for a lot of the "middle ground" of the spectrum between the "male" and "female" peaks. Any situation where easily assigning the person to one of those two peaks is challenging.
/25
"Intersex" is a grouping bin used for a lot of the "middle ground" of the spectrum between the "male" and "female" peaks. Any situation where easily assigning the person to one of those two peaks is challenging.
/25
Intersex! Because I didn't specifically mention this above.
"Intersex" is a term used to collectively speak of the "middle ground" of biology where people can't easily be binned into those two big "male" and "female" peaks. It can include a large range of biology
/27
"Intersex" is a term used to collectively speak of the "middle ground" of biology where people can't easily be binned into those two big "male" and "female" peaks. It can include a large range of biology
/27
It is worth noting that I never talk about transgender in this thread. Intersex is not the same as transgender. You can be one without the other, or be both.
/28
/28
For people who think this is just "outliers"
Current estimates are that the intersex population is at least 2%. We know that's low because there are a lot of "invisibly intersex" people. That means AT LEAST 150 million people in the world.
/29
Current estimates are that the intersex population is at least 2%. We know that's low because there are a lot of "invisibly intersex" people. That means AT LEAST 150 million people in the world.
/29
I apologize for the failure to use the word "intersex" higher up in the discussion. Many people in the middle ground (including the XY person who can carry a child, for example) use this term. I cannot go back and edit the thread, and apologize for my overly clinical description.
Part of the purpose of the thread, which may have failed, was to point out that "intersex" is not a condition, it is not a disease. It's natural with a bimodal distribution. Science not only supports this, it suggests that ignoring intersex people makes your conclusions wrong
For those curious to learn more about the less clinical "these things exist" side of intersex people, I recommend intersexroadshow.blogspot.com
Here is a solid explanation of the embryology of sex organs and how that relates to a sex spectrum and intersex people. intersexroadshow.blogspot.com/2011/01/phallo…
A human result of the scientific conclusion that sex is a spectrum and intersex people are a perfectly normal result of nature, is that there is no scientific rationale for medically (or culturally) forcing people into those two peaks.
A note here that I am muting the thread, not because I don't want to respond but because I did not expect it to blow up so much, and I have family and work to take care of. I'll try to wander back, but can't guarantee how much it will be.
Another addition, because a couple people have asked about it.
It's important to note that there are other people who traditionally haven't fallen into the "intersex" category, but also don't fall into the clearly defined peaks either.
It's important to note that there are other people who traditionally haven't fallen into the "intersex" category, but also don't fall into the clearly defined peaks either.
For example: XX people with female secondary sex characteristics, and ovaries who won't menstruate and can't carry a child without adding external (exogenous) estrogen. People like this often have difficulties finding good endocrinology care.
One more note here: This was meant to be an informational thread, based on my own data/experience as a scientist. I am not the be-all end-all of science and don't claim to be. There are rational scientists who disagree with me.
Neither, though, do I have time for a full-on scientific debate on Twitter. Maybe we can talk at an Endocrine Society meeting or something. Unfortunately, I do have a life and stuff to do. And Twitter pays no bills.
Many people have asked for reading and papers. This is an opinion piece, which I largely agree with, that references some of the more common human-based scientific papers people use to discuss this issue. Others interpret these same studies differently nature.com/news/sex-redef…
And one more note that "spectrum" does not mean that there aren't clusters of people. Just like the spectrum of human voice range has more baritones than super-bases.
Several people have asked about the physical structures of brains that differ between sex. This work ties in neatly with what I was saying above. There's many systems and pieces of physiology that each vary, along with the sum-brain/behavior that results. sciencemag.org/news/2015/11/b…
As this is twitter, and I'm not speaking as a representative of an institution or as part of my job, I have not shared proof of my credentials. I don't want to risk labs/schools I've worked with (or family) getting harassed when they didn't volunteer that information.
I know that makes things more difficult for those trying to do their research, but it's the reality of the platform.
But I can provide some more sources for those actually interested. They include some fairly heavy duty science, but some are open access/free for all
But I can provide some more sources for those actually interested. They include some fairly heavy duty science, but some are open access/free for all
Sources:
These deal with the fact that the sexually dimorphic brain, similar to most sex differences, does not fall into a hard binary readout - but rather is on a continuum or spectrum with each cell and each brain region comprised of varying degrees of ‘male' and ‘female'
These deal with the fact that the sexually dimorphic brain, similar to most sex differences, does not fall into a hard binary readout - but rather is on a continuum or spectrum with each cell and each brain region comprised of varying degrees of ‘male' and ‘female'
Hines M (2005). Brain Gender. Oxford University Press: Oxford
Joel D, McCarthy MM (2016). Incorporating sex as a biological variable in neuropsychiatric research: where are we now and where should we be? Neuropsychopharmacology ncbi.nlm.nih.gov/pubmed/27240659
Joel D, McCarthy MM (2016). Incorporating sex as a biological variable in neuropsychiatric research: where are we now and where should we be? Neuropsychopharmacology ncbi.nlm.nih.gov/pubmed/27240659
This paper deals with the complications of epigenetics that can divert the genetic sex and gonadal hormone pathways in subtle ways to produce large trajectory changes. Epigenetics plays a large role in estrogenic apoptosis via DNA methylation.
Gregg C, Zhang J, Weissbourd B, Luo S, Schroth GP, Haig D et al (2010). High-resolution analysis of parent-of-origin allelic expression in the mouse brain. Science 329: 643–648
ncbi.nlm.nih.gov/pubmed/20616232
ncbi.nlm.nih.gov/pubmed/20616232
This one with the interactions between social experience and biology
Springer KW, Mager Stellman J, Jordan-Young RM (2012). Beyond a catalogue of differences: a theoretical frame and good practice guidelines for researching sex/gender in human health. Soc Sci Med 74: 1817–1824
Springer KW, Mager Stellman J, Jordan-Young RM (2012). Beyond a catalogue of differences: a theoretical frame and good practice guidelines for researching sex/gender in human health. Soc Sci Med 74: 1817–1824
@threadreaderapp unroll please and thank you
And one on the heterogeneity of brains:
Joel & Sterling 2016. Beyond sex differences: new approaches for thinking about variation in brain structure and function. Philos Trans R Soc Lond B Biol Sci. 2016 Feb 19; 371(1688)
ncbi.nlm.nih.gov/pmc/articles/P…
Joel & Sterling 2016. Beyond sex differences: new approaches for thinking about variation in brain structure and function. Philos Trans R Soc Lond B Biol Sci. 2016 Feb 19; 371(1688)
ncbi.nlm.nih.gov/pmc/articles/P…
• • •
Missing some Tweet in this thread? You can try to
force a refresh