
1/How does primary aldosteronism present? When should you look for it?
Here are a couple of clinical cases I like to share with audiences when I talk about the severity spectrum of primary aldosteronism, and the many ways autonomous aldosterone secretion can manifest.
Here are a couple of clinical cases I like to share with audiences when I talk about the severity spectrum of primary aldosteronism, and the many ways autonomous aldosterone secretion can manifest.
2/Here are two patients. 

3/
Would you screen for primary aldosteronism?
Would you screen for primary aldosteronism?
4/
Case 1 = YES. He has chronic HTN, uncontrolled on 4 drugs, and hypoK.
Case 2 = Prob not? This patient would’ve been “normotensive” in the past, but in 2018, he has HTN. His PCP starts him on chlorthalidone and 2 weeks later his K=2.9.
Case 1 = YES. He has chronic HTN, uncontrolled on 4 drugs, and hypoK.
Case 2 = Prob not? This patient would’ve been “normotensive” in the past, but in 2018, he has HTN. His PCP starts him on chlorthalidone and 2 weeks later his K=2.9.

5/
Would you screen Case 2 for primary aldosteronism now?
Would you screen Case 2 for primary aldosteronism now?
6/
YES. Diuretic-induced hypokalemia is an indication to screen for PA
ncbi.nlm.nih.gov/pubmed/28332881
YES. Diuretic-induced hypokalemia is an indication to screen for PA
ncbi.nlm.nih.gov/pubmed/28332881

7/
Both patients are screened for PA, see results.
Both patients are screened for PA, see results.

8/ Could these patients have primary aldosteronism?
9/
Case 1: YES/CONFIRMED. HypoK, suppressed renin, very high aldosterone. This is a positive screen and positive confirmation.
Case 2: YES/POSSIBLY. Normal K. suppressed renin. But ?inappropriately elevated? aldosterone?
Case 1: YES/CONFIRMED. HypoK, suppressed renin, very high aldosterone. This is a positive screen and positive confirmation.
Case 2: YES/POSSIBLY. Normal K. suppressed renin. But ?inappropriately elevated? aldosterone?

10/
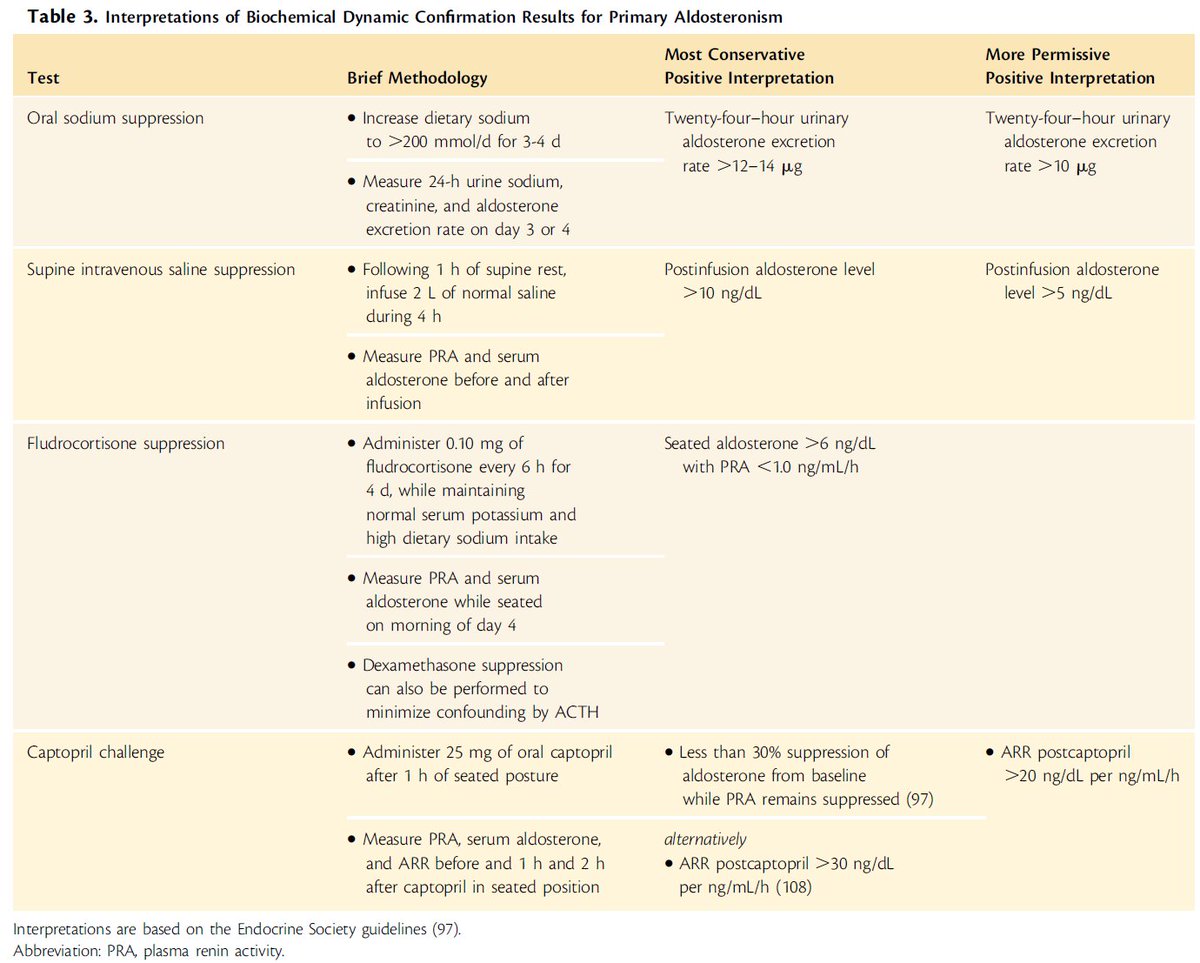
Case 2 undergoes a confirmatory oral sodium suppression test (4 days of high sodium diet). 24h UNa>200 mmol and 24h aldosterone excretion rate = 16 mcg/24h
Case 2 undergoes a confirmatory oral sodium suppression test (4 days of high sodium diet). 24h UNa>200 mmol and 24h aldosterone excretion rate = 16 mcg/24h

11/
Does Case 2 have primary aldosteronism?
Does Case 2 have primary aldosteronism?
12/
YES, they both have PA.
Case 1 was obvious, prob could have been diagnosed years/decades earlier.
Case 2 was diagnosed early and will hopefully avoid years of CV disease.
One diagnostic approach w/flexibility to detect cases of varying severity =>
ncbi.nlm.nih.gov/pubmed/30124805
YES, they both have PA.
Case 1 was obvious, prob could have been diagnosed years/decades earlier.
Case 2 was diagnosed early and will hopefully avoid years of CV disease.
One diagnostic approach w/flexibility to detect cases of varying severity =>
ncbi.nlm.nih.gov/pubmed/30124805

13/
Final thoughts:
Exact prevalence not completely clear, but primary aldosteronism can be detected in severe/resistant HTN (>10%), mild-mod HTN (~4-10%)…
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=1…
Final thoughts:
Exact prevalence not completely clear, but primary aldosteronism can be detected in severe/resistant HTN (>10%), mild-mod HTN (~4-10%)…
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=1…
14/
As well as among normotensives (who have a higher risk for developing overt HTN).
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=2…
Much more work needed to determine how to expand screening in an effective way to detect PA early/end
As well as among normotensives (who have a higher risk for developing overt HTN).
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=2…
ncbi.nlm.nih.gov/pubmed/?term=2…
Much more work needed to determine how to expand screening in an effective way to detect PA early/end
15/ For more on primary aldosteronism => see final version of our comprehensive, contemporary (and colorful!) review. We review the history of aldosteronism, and the latest in diagnosis, pathogenesis, and treatment...
ncbi.nlm.nih.gov/pubmed/30124805
ncbi.nlm.nih.gov/pubmed/30124805

16/ ….approaching the diagnosis of primary aldosteronism…


17/ …current theories on the pathogenesis and severity spectrum of primary aldosteronism…

18/ …recent evidence and opinions on treatment of primary aldosteronism…


19/ Many thanks to #EndocrineReviews @EndoSocJournals @DanielJDrucker for the opportunity, the wordspace, and medical illustration to bring our figures to life!
• • •
Missing some Tweet in this thread? You can try to
force a refresh




