Another small addition here...
I've gotten critiques saying that I'm claiming intersex people "aren't real men or women." That's NOT what the data says. What the data says is that the labels "real men" and "real women" are not accurate labels for ANYONE.
I've gotten critiques saying that I'm claiming intersex people "aren't real men or women." That's NOT what the data says. What the data says is that the labels "real men" and "real women" are not accurate labels for ANYONE.
For example, outside of the more obvious cases, I naturally have a significantly lower resting testosterone level than my brother. This means a lot of things. It means I'm likely to respond differently to hormones or mimics/disruptors.
Give us both testosterone (or estrogen, or a bisphenol) and the results would be different. It doesn't make him or me a "real" man, it means we're in different places along the response curve. It means that "real" is an arbitrary line we've drawn.
Something new on the research end, is that it looks like sex phenotype has to be MAINTAINED in adulthood. That's actually a pretty huge change in our understanding. There's a gene that's required to keep your body the way it is.
ovaries/testes have to be maintained in adulthood and can change with changes in the right genes
Sex determination and maintenance: the role of DMRT1 and FOXL2
Huang et al, 2017
ncbi.nlm.nih.gov/pmc/articles/P…
Sex determination and maintenance: the role of DMRT1 and FOXL2
Huang et al, 2017
ncbi.nlm.nih.gov/pmc/articles/P…
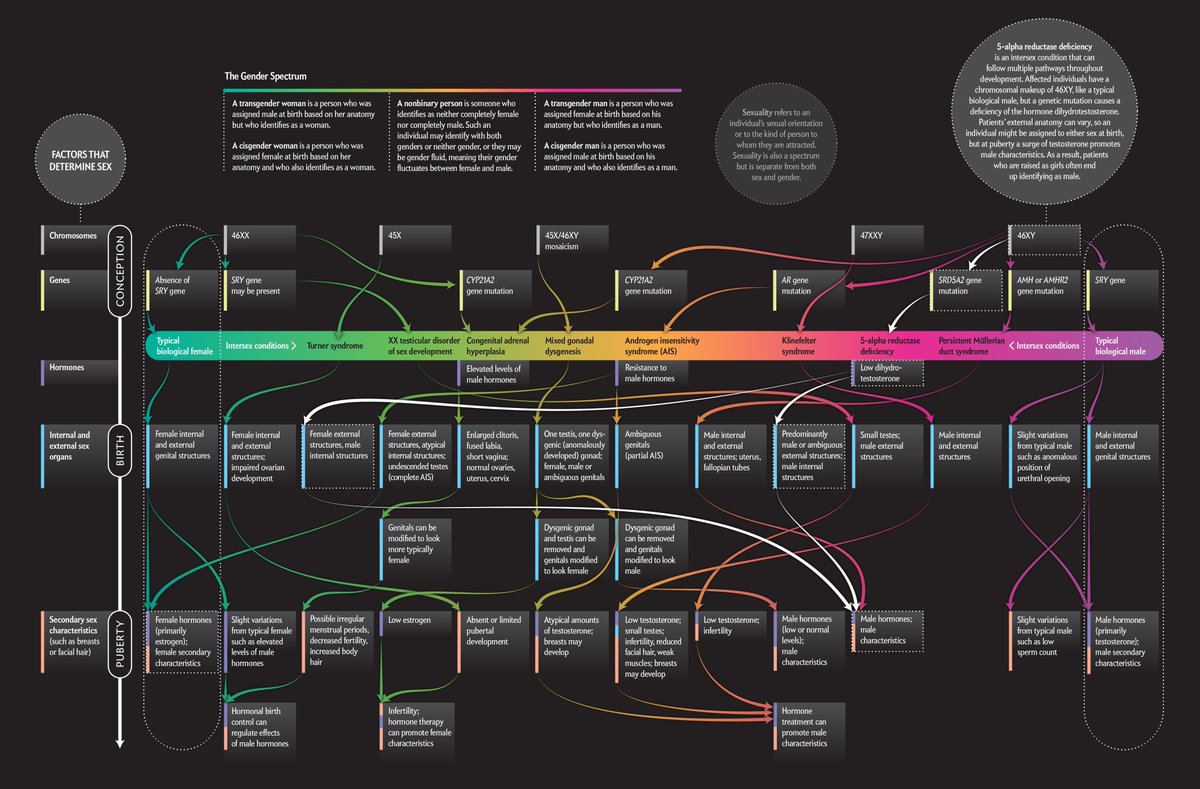
A graphic of SOME of the things that can shift sex determination around in humans. This doesn't get into some of the newer things like DMRT1 or FOXL2. But it gives you an idea of how many different paths there are even if we just look at base chromosomes/genes 
Another example. We've discovered there's a larger group than thought of "late-onset congenital adrenal hyperplasia." The default for these women has been to supplement with estrogen/progesterone. For some it works, but for many it can cause suicidal depression.
i.e. trying to treat these women in the "there are two and only two" model - by trying to make their body chemistry match an idealized model - not only doesn't work, it can kill them.
This article does a decent job of encompassing a lot of the more recent discoveries. It also does a better job than most about talking about the non-obvious non-intersex parts of the continuum such as "non-classical" CAH.
scientificamerican.com/article/sex-re…
scientificamerican.com/article/sex-re…
It's important to talk about the non-obvious parts of the spectrum, as the people just a few steps out from the peaks of the curve can be hugely damaged if medicine doesn't account for the difference. And since it's easier not to, doctors often don't.
Local maxima/minima do not disprove a spectrum. I.e. if the world were mostly blue and red, it wouldn't disprove that there is a spectrum of light.
This article has a ton of good links to primary sources, and does a good job of talking about how the spectrum extends past the "obvious" points and providing examples of how it appears even in those two big peaks at the ends.
blogs.scientificamerican.com/voices/stop-us…
blogs.scientificamerican.com/voices/stop-us…
• • •
Missing some Tweet in this thread? You can try to
force a refresh