
32/F, 12 wks pregnant p/w malaise and rash. Exam: diffuse maculopapular rash including palms/soles. HIV (-), RPR 1:128. No prior h/o STIs or other PMH. No headache, blurred vision, normal neuro exam. No genital lesion. Most appropriate treatment? #IDMedEd #syphilis
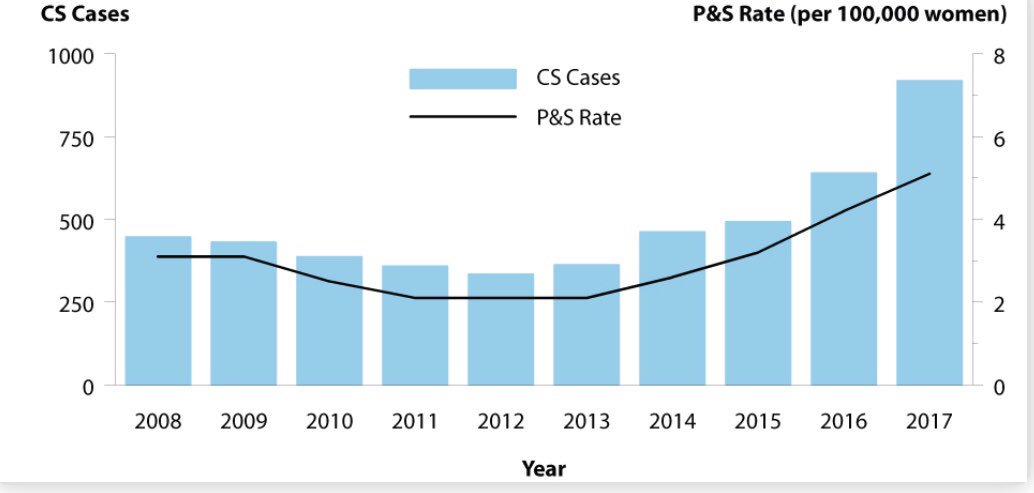
(1/11) The correct answers are A (34%) & B (13%). Note case should’ve mentioned +confirmatory test. Cases of congenital syphils >doubled from 2013 (362 cases) to 2017 (918 cases), coincident w/ the rise in primary & secondary syphils rates among all women cdc.gov/std/stats17/sy… 
(2/11) Untreated maternal syphilis, in up to ✔️80% of cases, leads to severe adverse pregnancy outcomes (congenital infection, stillbirth, premature birth, neonatal death). #IDMedEd #syphilis
(3/11) PCN is the 🌟ONLY effective Tx for preventing congenital transmission. PCN remains the DOC for syphilis. TP remarkably has not developed PCN resistance over time unlike other bugs. This @tony_breu tweetorial on why this is so is 🌟highly recommended
https://twitter.com/tony_breu/status/1015993557403033601?s=21
(4/11) Pregnant women with syphilis should be treated 📌ACCORDING to their stage of infection. Remember, neurosyphilis can occur during 🌟ANY stage. Thus, a good history and physical/neuro exam are essential in diagnosing and treating syphilis appropriately. #IDMedEd
(5/11) In our case, the diffuse MP rash involving palms/soles is a hallmark of 🌟secondary syphilis. Have you wondered why syphilis rash loves to involve the palms/soles (& why the lesion is painless)? I highly recommend this tweetorial #IDMedEd @tony_breu
https://twitter.com/tony_breu/status/1116386861608505344?s=21
(6/11) PCN x 1 (2.4 M units) is a correct answer here (standard Tx of primary, secondary & early latent stage syphilis). The CDC guideline also highlights the benefit of a 2nd dose of 2.4 M units 1 wk after the initial dose among ✔️pregnant women #IDMedEd cdc.gov/std/tg2015/syp…
(7/11) Note that the 2nd dose of PCN for early stage syphilis among pregnant women as acknowledged by the CDC guidline is based on expert opinion derived from PCN pharmacokinetic data during pregnancy and studies that showed benefit. #IDMedEd ncbi.nlm.nih.gov/m/pubmed/12353…
(8/11) Note that the WHO and European guidelines recommend single PCN dose for the Tx of early syphilis among pregnant women: who.int/reproductivehe… & iusti.org/regions/europe…
(9/11) When syphilis is dx during the 2nd half of pregnancy, fetal US should be performed to evaluate for congenital syphilis. #IDMedEd #syphilis
(10/11) If Tx results to Jarisch-Herxheimer in women tx during the 2nd half of pregnancy, can be at risk of premature labor (increased awareness of symptoms & obstetric attention needed; stillbirth rare but concern for this should not delay necessary Tx) cdc.gov/std/tg2015/syp…
(11/11) Let’s hear more from our syphilis expert @hrenoID regarding screening and treatment of maternal syphilis & prevention of congenital transmission. #IDMedEd #syphilis
• • •
Missing some Tweet in this thread? You can try to
force a refresh




