With a crop of new interns hitting the wards tomorrow, here are ten (somewhat random) #TipsForNewDocs with a focus on drugs. Feel free to suggest others.
Thread —>
Thread —>
1. Most patients who report a penicillin allergy don’t actually have one. Rather than blanket avoidance, use the history to guide your approach. jamanetwork.com/journals/jama/… by @ericashenoy, @EricMacyMD et al. 

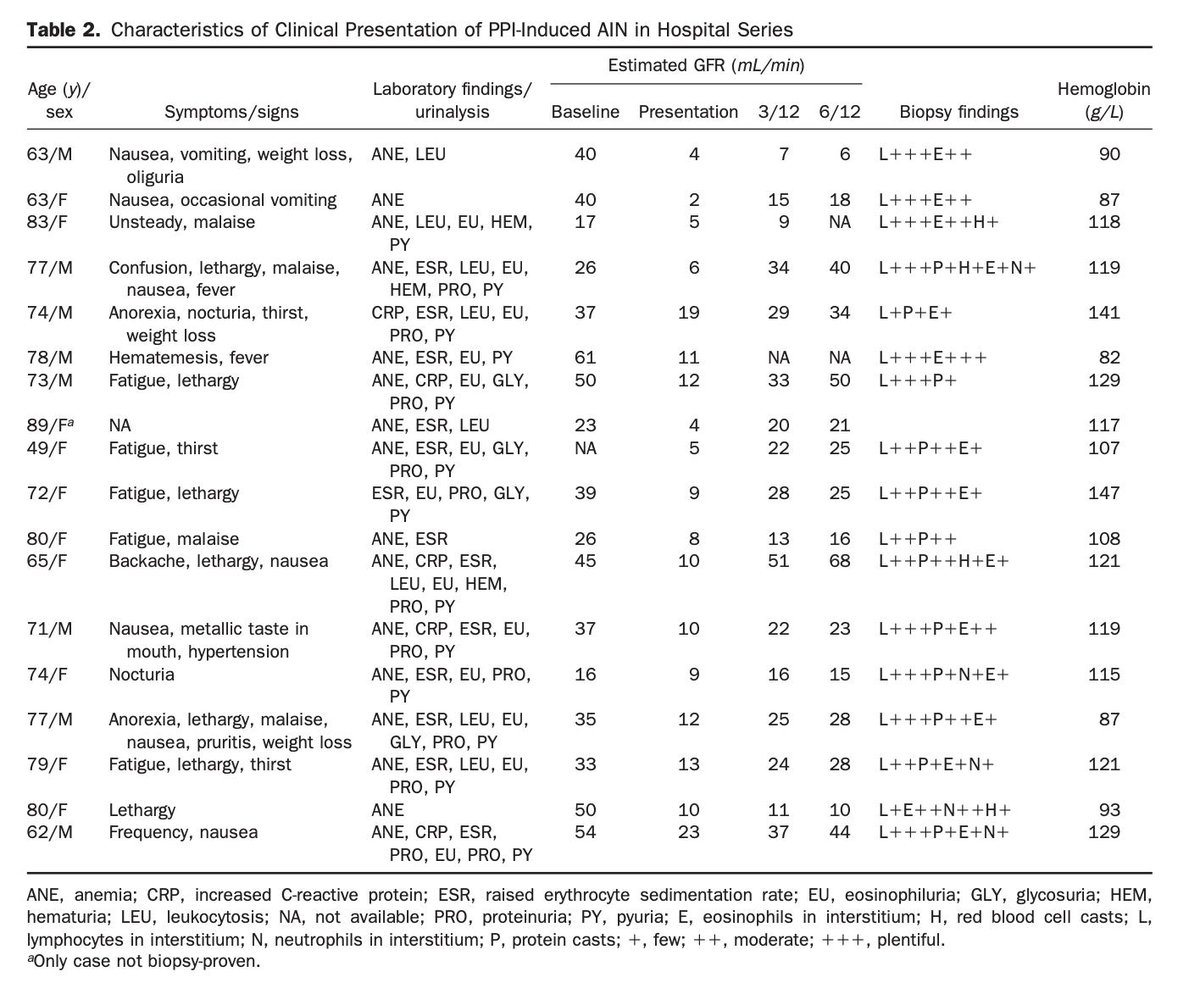
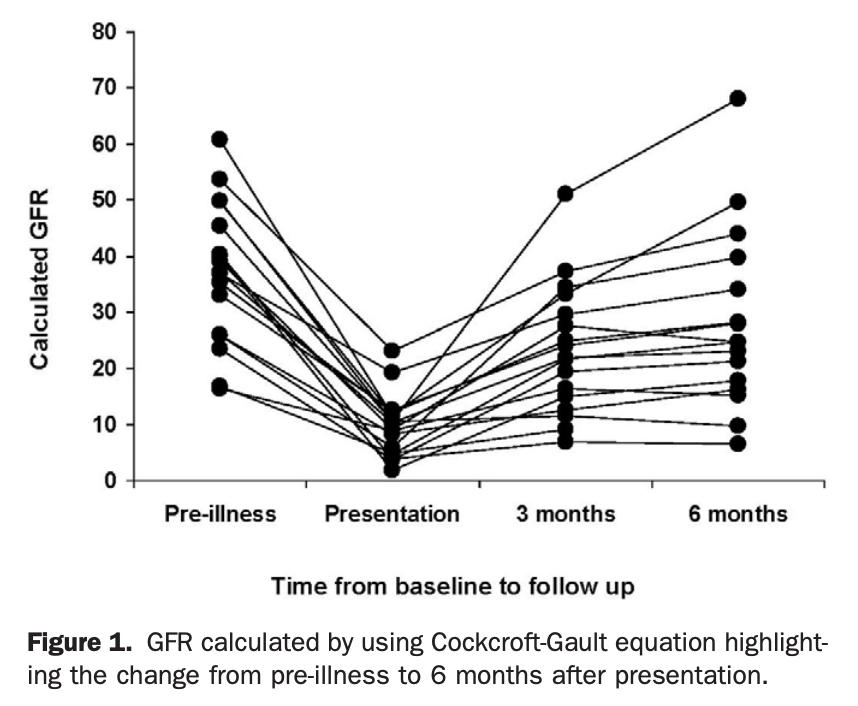
2. Not sure why the creatinine is up? Consider drug-induced AIN, and PPIs in particular because of how widely used they are. The presentation is bland and easily missed. cghjournal.org/article/S1542-…
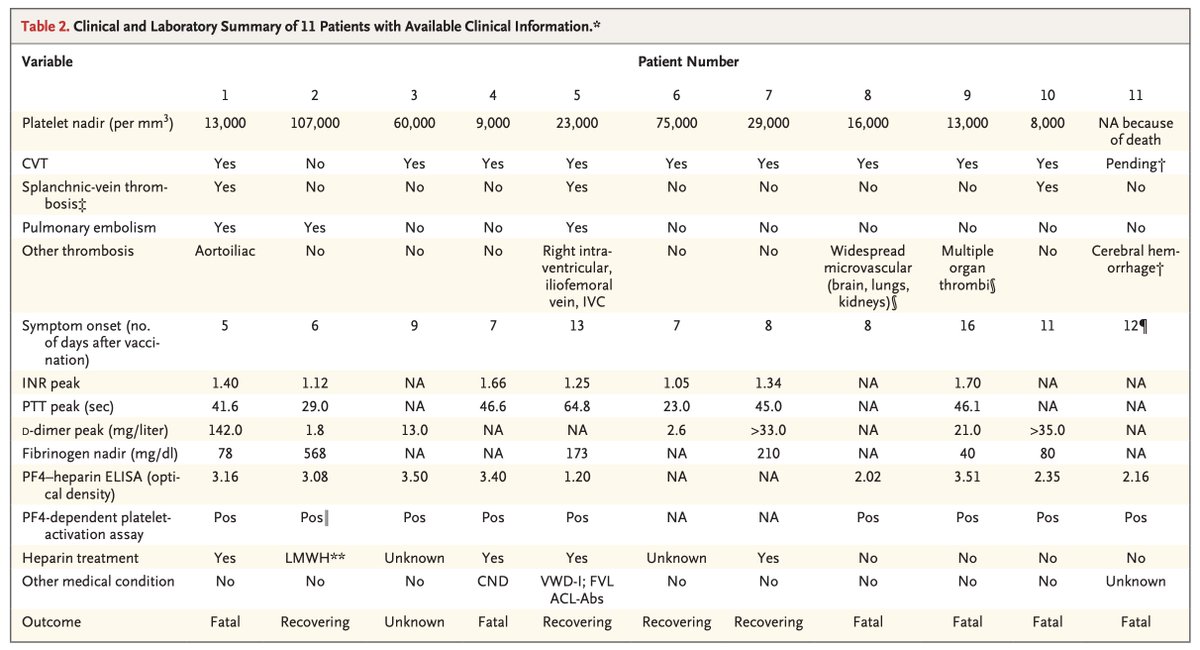
3. Is it serotonin syndrome or NMS? You can usually tell before entering the room. Boils down to drug history (D2 antagonists vs. 5-HT2A agonists) and the time course of illness (rapid vs. gradual & fluctuating) mhc.cpnp.org/doi/full/10.97…

3a) On exam, serotonin syndrome is all about the clonus
https://twitter.com/DavidJuurlink/status/1133033294428364800
4. When treating pain, you have more options at your disposal than you might appreciate, especially in hospitalized patients. Ketamine in particular is your friend. linkinghub.elsevier.com/retrieve/pii/S… by @emupdates, @LNelsonMD & @painfreeED


4a) A comment on “weak opioids”:
- Don’t use codeine. It’s an inert prodrug metabolized unpredictably to morphine. Just give morphine.
- As for tramadol, well … emcrit.org/toxhound/trama…
- Don’t use codeine. It’s an inert prodrug metabolized unpredictably to morphine. Just give morphine.
- As for tramadol, well … emcrit.org/toxhound/trama…
5. Rash + fever? Might be delayed hypersensitivity. Ask about drugs started in the preceding ~6 weeks, especially:
- antibiotics (esp. B-lactams, sulfas, vanco)
- anticonvulsants
- NSAIDs
- allopurinol
- dapsone
And sure, look for eosinophilia. But lymphopenia is more common.
- antibiotics (esp. B-lactams, sulfas, vanco)
- anticonvulsants
- NSAIDs
- allopurinol
- dapsone
And sure, look for eosinophilia. But lymphopenia is more common.
6. INR all over the map in a patient on warfarin? Maybe it’s acetaminophen.
https://twitter.com/DavidJuurlink/status/782611855089004544
7. Managing sulfonylurea-induced hypoglycemia? Using IV dextrose alone is just asking for rebound hypoglycemia. Octreotide, OTOH, is magic. annemergmed.com/article/S0196-…

8. Trimethoprim-induced hyperkalemia can literally kill people.
Especially those already taking ACEIs, ARBs or spironolactone.
Especially those already taking ACEIs, ARBs or spironolactone.
https://twitter.com/DavidJuurlink/status/1018498915656749056
9. Drugs that can produce withdrawal syndromes (benzos, opioids, baclofen, clonidine, pregabalin & others) should not be started lightly. If you’re planning to use them for more than a few days, have a plan for tapering. Don't stop them abruptly.
10. Before ordering a urine drug screen, place the index finger of your dominant hand in a stapler and press down firmly. If you still want to order one thereafter, go right ahead.
/ end (additions welcome)
/ end (additions welcome)
11. Pharmacists: They'll save your ass.ᵀᴹ
https://twitter.com/kplant_gnv/status/1145678611309113351
• • •
Missing some Tweet in this thread? You can try to
force a refresh