
Yes, the AstraZeneca vaccine-thrombosis association is causal.
The temporal relationship is strong, it’s not seen with mRNA vaccines, and there’s a plausible mechanism analogous to heparin-induced thrombocytopenia (HIT)
nejm.org/doi/full/10.10…
The temporal relationship is strong, it’s not seen with mRNA vaccines, and there’s a plausible mechanism analogous to heparin-induced thrombocytopenia (HIT)
nejm.org/doi/full/10.10…
As with HIT, these are unusual clots: they occur in odd places (brain, abdomen) and in arteries as well as veins.
They’re more serious than the run-of-the mill clots we see all the time.
They’re more serious than the run-of-the mill clots we see all the time.
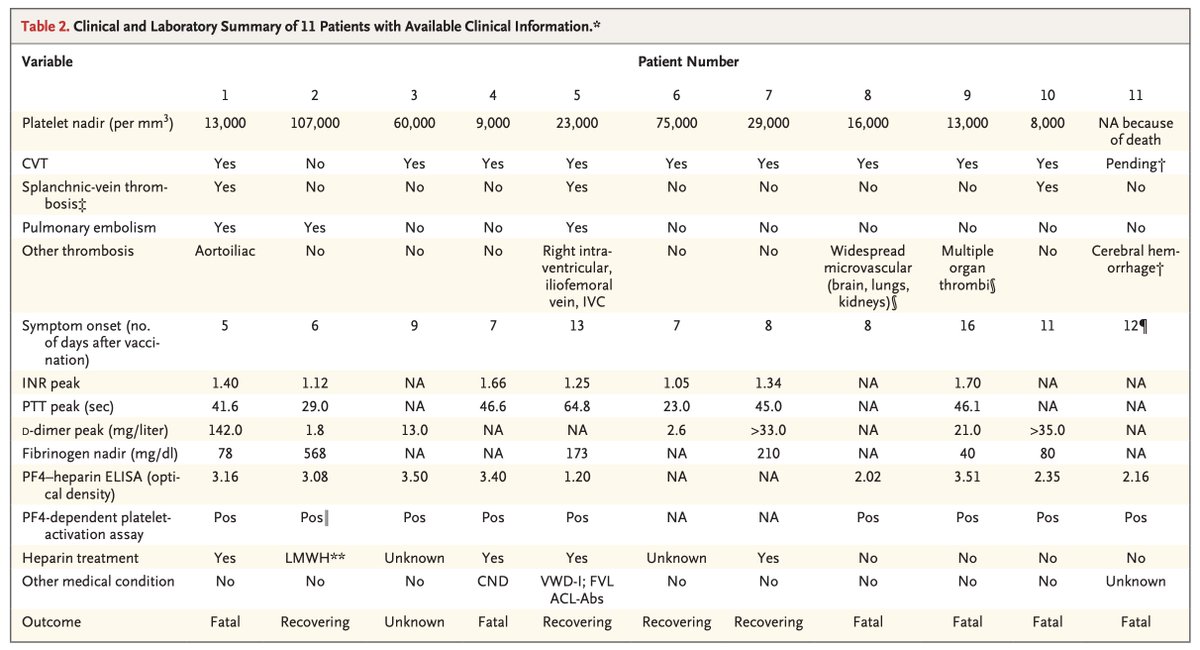
What's the risk? This has been a bit of a moving target, but it seems to be on the order of 1 in 100,000.
It's possible some cases have been missed, especially in older people.
Still, fair to call it very rare.
It's possible some cases have been missed, especially in older people.
Still, fair to call it very rare.
With all the buzz and mixed messaging around this issue, many are now reluctant to receive the AZ vaccine.
This is understandable. People are risk-averse by nature.
But it's important to view the risk in context.
This is understandable. People are risk-averse by nature.
But it's important to view the risk in context.
“I’ll pass on the vaccine. My risk of dying from COVID is low."
This is a take I've heard more than once.
This framing is faulty because it neglects the other downsides of COVID—hospitalization, spending a week or more on a ventilator, and so on.
This is a take I've heard more than once.
This framing is faulty because it neglects the other downsides of COVID—hospitalization, spending a week or more on a ventilator, and so on.
Your risk of a bad outcome with COVID depends heavily on two things: your age, and your likelihood of contracting the virus in the first place.
You're 25 and living in a Unabomber-style cabin in rural Montana? By all means, take a pass.
You're 25 and living in a Unabomber-style cabin in rural Montana? By all means, take a pass.
You're 61 and living in Toronto? Different story altogether.
Especially if you spend a lot of time around others, either at work or home.
Especially if you spend a lot of time around others, either at work or home.
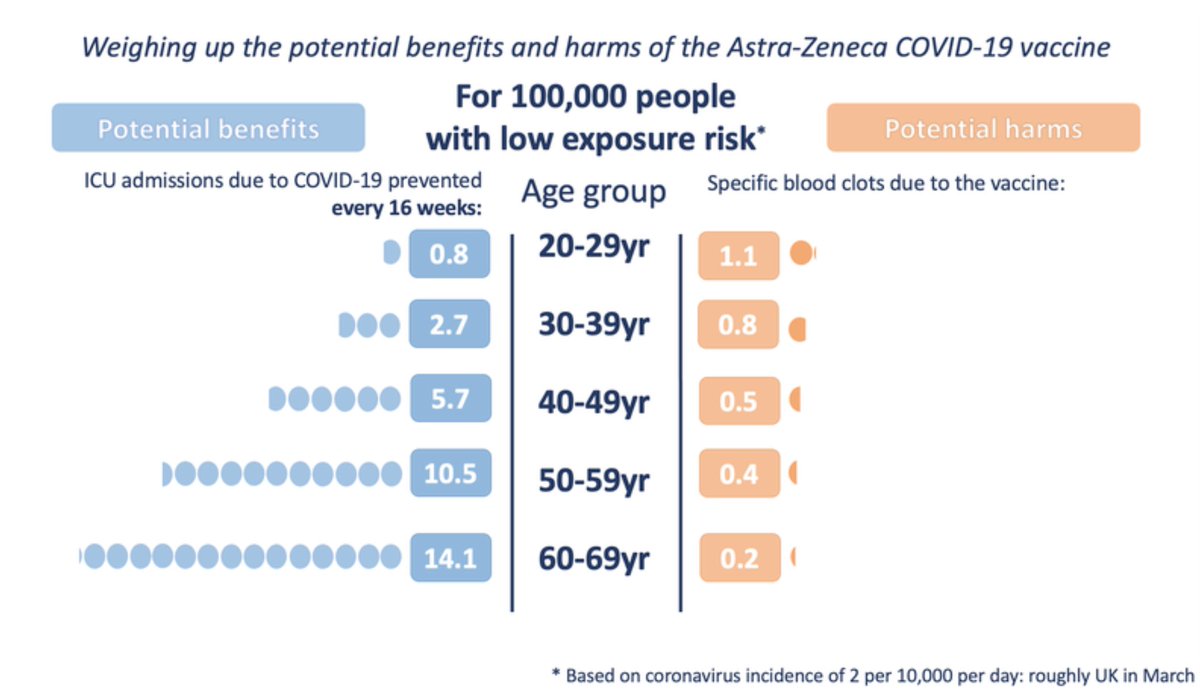
To weigh the risks and benefits for yourself, it's worth checking out this resource from the Winton Centre for Risk and Evidence Communication (not on Twitter, apparently) at @Cambridge_Uni
wintoncentre.maths.cam.ac.uk/news/communica…
wintoncentre.maths.cam.ac.uk/news/communica…
Here's their assessment of the potential benefits and harms by age when the risk of exposure is low
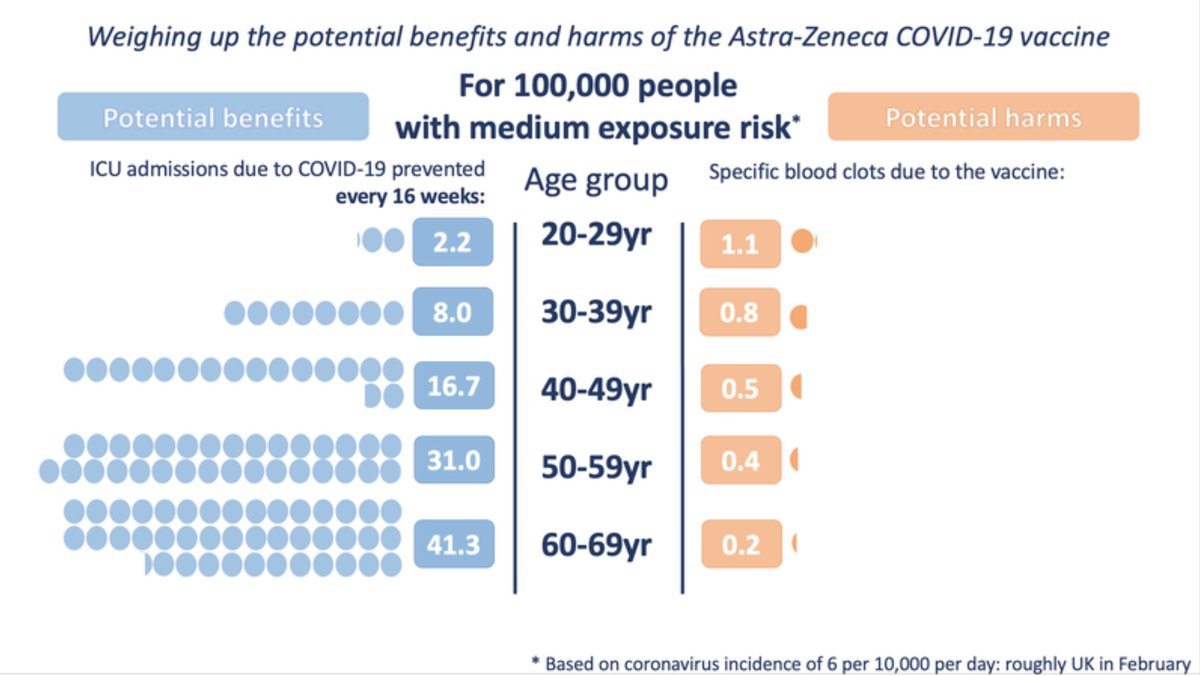
Here's the calculus when the risk of exposure increases to "medium"
And here's when the risk of exposure is high
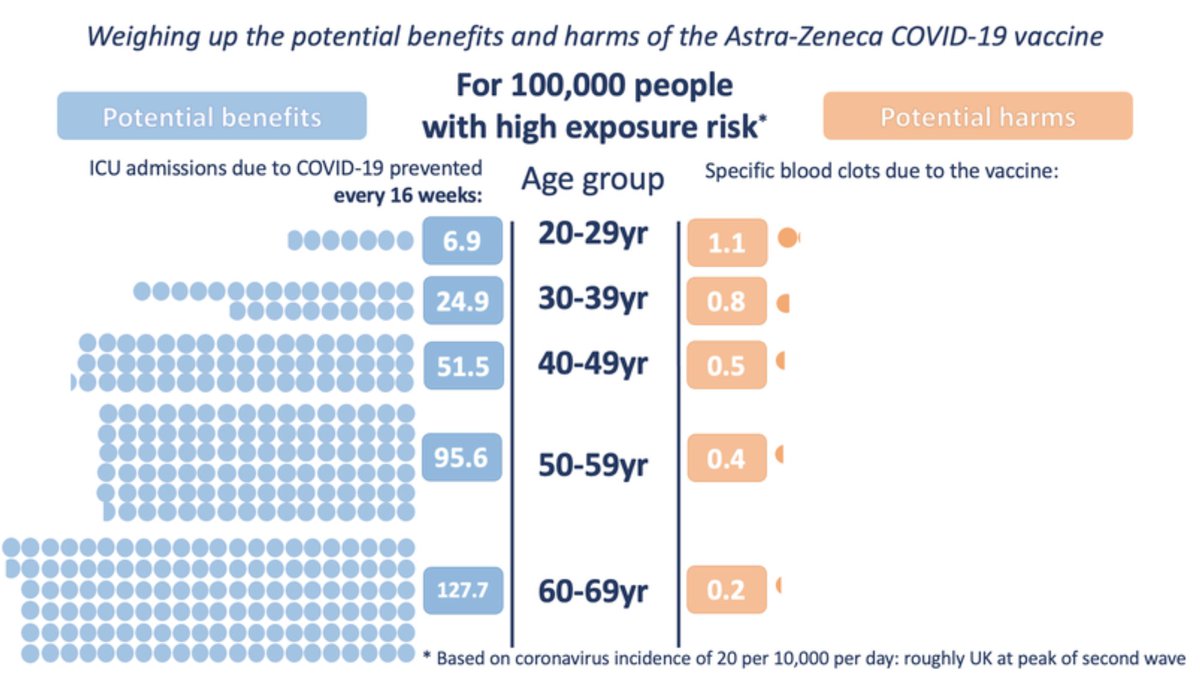
Reasonable people can disagree on the age threshold below which the potential risk of an unusual clot isn't worth the potential benefits of vaccination.
Even regulators disagree on this.
Even regulators disagree on this.
https://twitter.com/jburnmurdoch/status/1379802402367373315?s=20
Anyway, my point is don't be spooked by scary headlines and mixed messages.
Every drug has potential harms, and the AZ vaccine is no different. It's just important to place them in context.
/ end
Every drug has potential harms, and the AZ vaccine is no different. It's just important to place them in context.
/ end
• • •
Missing some Tweet in this thread? You can try to
force a refresh





