
ID Miscellany|physical Exam|Signs|Humanities #idmesh
1/7
𝐄𝐩𝐢𝐭𝐫𝐨𝐜𝐡𝐥𝐞𝐚𝐫 𝐍𝐨𝐝𝐞𝐬
Palpating for the epitrochlear nodes is an exam that I like to teach at bedside. When palpable, these nodes often indicate a condition characterized by generalized lymphadenopathy.
1/7
𝐄𝐩𝐢𝐭𝐫𝐨𝐜𝐡𝐥𝐞𝐚𝐫 𝐍𝐨𝐝𝐞𝐬
Palpating for the epitrochlear nodes is an exam that I like to teach at bedside. When palpable, these nodes often indicate a condition characterized by generalized lymphadenopathy.
2/7
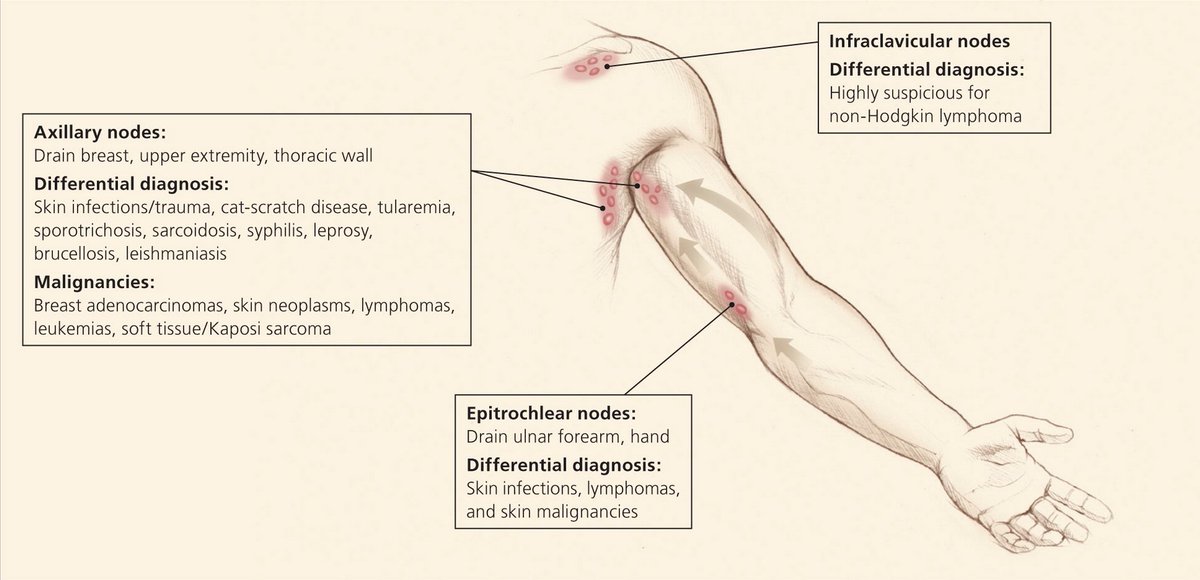
Epitrochlear nodes (EN) are superficial nodes located 2-3 cm above and anterior to the medial condyle of the humerus.
Exam: shake patient's hand, on the side to be examined; examiner's free hand palpates for ENs 👇
Pics from:
aafp.org/afp/2016/1201/…
memorangapp.com/flashcards/802…
Epitrochlear nodes (EN) are superficial nodes located 2-3 cm above and anterior to the medial condyle of the humerus.
Exam: shake patient's hand, on the side to be examined; examiner's free hand palpates for ENs 👇
Pics from:
aafp.org/afp/2016/1201/…
memorangapp.com/flashcards/802…

3/7
ENs drain the ulnar forearm & the little/ring fingers.
Enlarged ENs are rare in healthy individuals (no more than few millimeters in size).
Unilateral enlargement can indicate localized cutaneous infection/malignancy/inflammation of the forearm/hands.
ENs drain the ulnar forearm & the little/ring fingers.
Enlarged ENs are rare in healthy individuals (no more than few millimeters in size).
Unilateral enlargement can indicate localized cutaneous infection/malignancy/inflammation of the forearm/hands.
4/7
𝐒𝐲𝐦𝐦𝐞𝐭𝐫𝐢𝐜 𝐞𝐧𝐥𝐚𝐫𝐠𝐞𝐦𝐞𝐧𝐭 indicates a condition characterized by generalized LAD.
Historically, a/w secondary syphilis (at least 1/2 of cases).
jamanetwork.com/journals/jamad…
sciencedirect.com/science/articl…
Osler's two-handed hand-elbow salutation:
bmj.com/rapid-response…
𝐒𝐲𝐦𝐦𝐞𝐭𝐫𝐢𝐜 𝐞𝐧𝐥𝐚𝐫𝐠𝐞𝐦𝐞𝐧𝐭 indicates a condition characterized by generalized LAD.
Historically, a/w secondary syphilis (at least 1/2 of cases).
jamanetwork.com/journals/jamad…
sciencedirect.com/science/articl…
Osler's two-handed hand-elbow salutation:
bmj.com/rapid-response…
5/7
They can also be seen in:
▪️ Mononucleosis & HIV (>50%)
▪️ Lymphoma, CLL, sarcoidosis (30%)
▪️ Rheumatoid arthritis (20%)
ncbi.nlm.nih.gov/pubmed/1588523
They can also be seen in:
▪️ Mononucleosis & HIV (>50%)
▪️ Lymphoma, CLL, sarcoidosis (30%)
▪️ Rheumatoid arthritis (20%)
ncbi.nlm.nih.gov/pubmed/1588523

6/7
A more recent review, however, shows us a wider range of disease associations 👇.
This review also identified:
▪️ leprosy as most commonly associated pre-HIV
▪️ HIV +/- TB, HIV pre-HAART era
▪️ cat-scratch disease, most common infection post-HAART
ncbi.nlm.nih.gov/pmc/articles/P…
A more recent review, however, shows us a wider range of disease associations 👇.
This review also identified:
▪️ leprosy as most commonly associated pre-HIV
▪️ HIV +/- TB, HIV pre-HAART era
▪️ cat-scratch disease, most common infection post-HAART
ncbi.nlm.nih.gov/pmc/articles/P…

7/7
Do you routinely palpate for epitrochlear nodes in your practice? Have you had opportunities that demonstrated its utility? Please feel free to leave your comments.
@AndreMansoor @DxRxEdu @TxID_Edu @BradCutrellMD @DocWoc71 @Darcy_ID_doc @MohitHarshMD
Do you routinely palpate for epitrochlear nodes in your practice? Have you had opportunities that demonstrated its utility? Please feel free to leave your comments.
@AndreMansoor @DxRxEdu @TxID_Edu @BradCutrellMD @DocWoc71 @Darcy_ID_doc @MohitHarshMD
• • •
Missing some Tweet in this thread? You can try to
force a refresh




