Why the 2019 @BLS_gov Jobs report is a red flag for American #healthcare: bls.gov/news.release/e…
A thread to explain
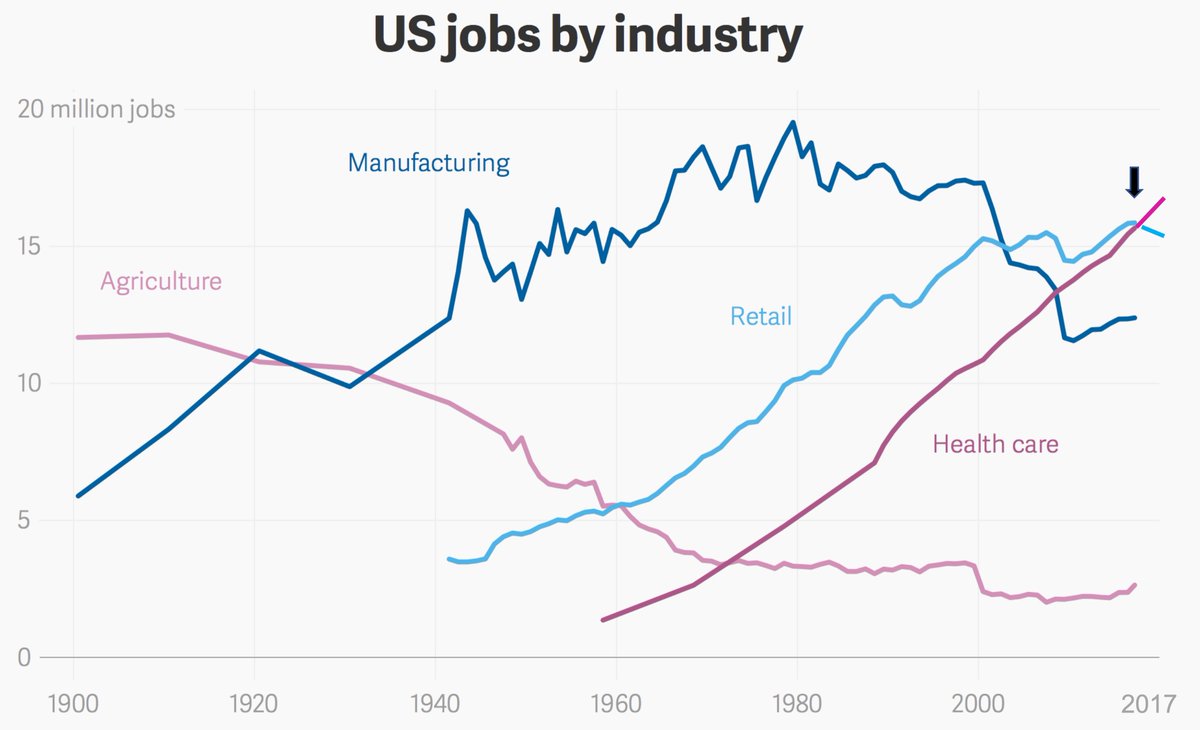
1. You may recall that in late December 2017, #healthcare jobs overtook retail to become #1 for the first time in US history
A thread to explain
1. You may recall that in late December 2017, #healthcare jobs overtook retail to become #1 for the first time in US history
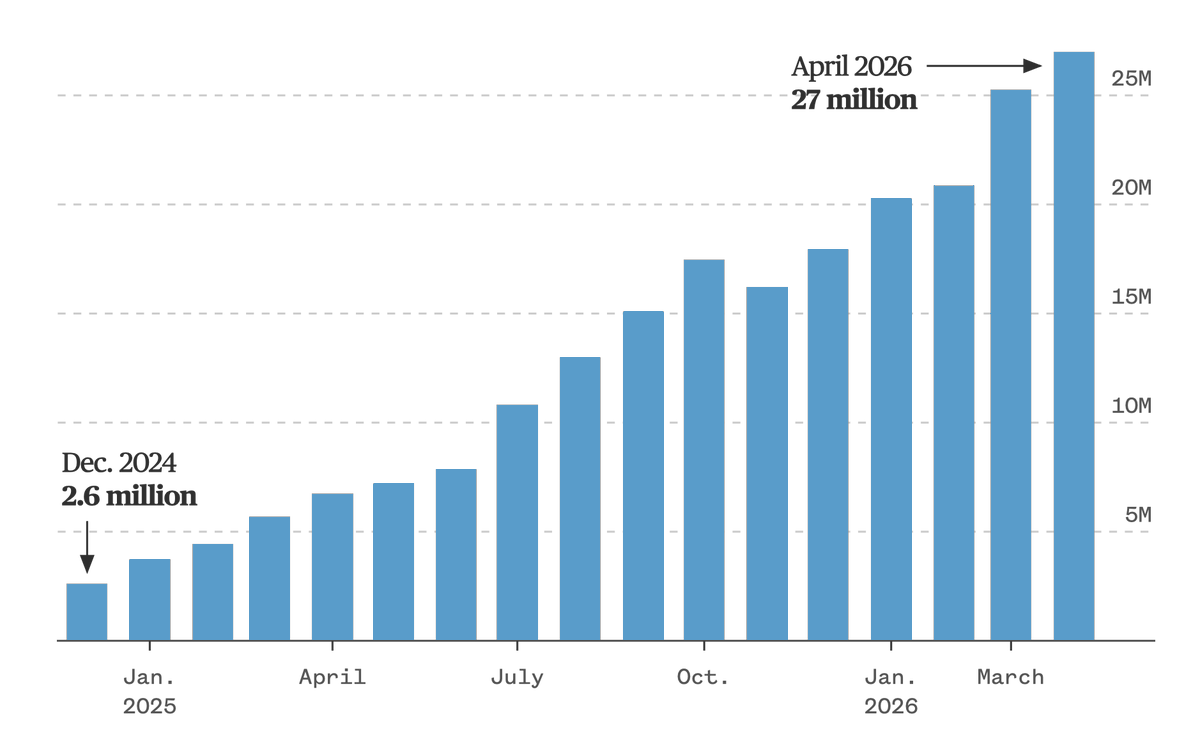
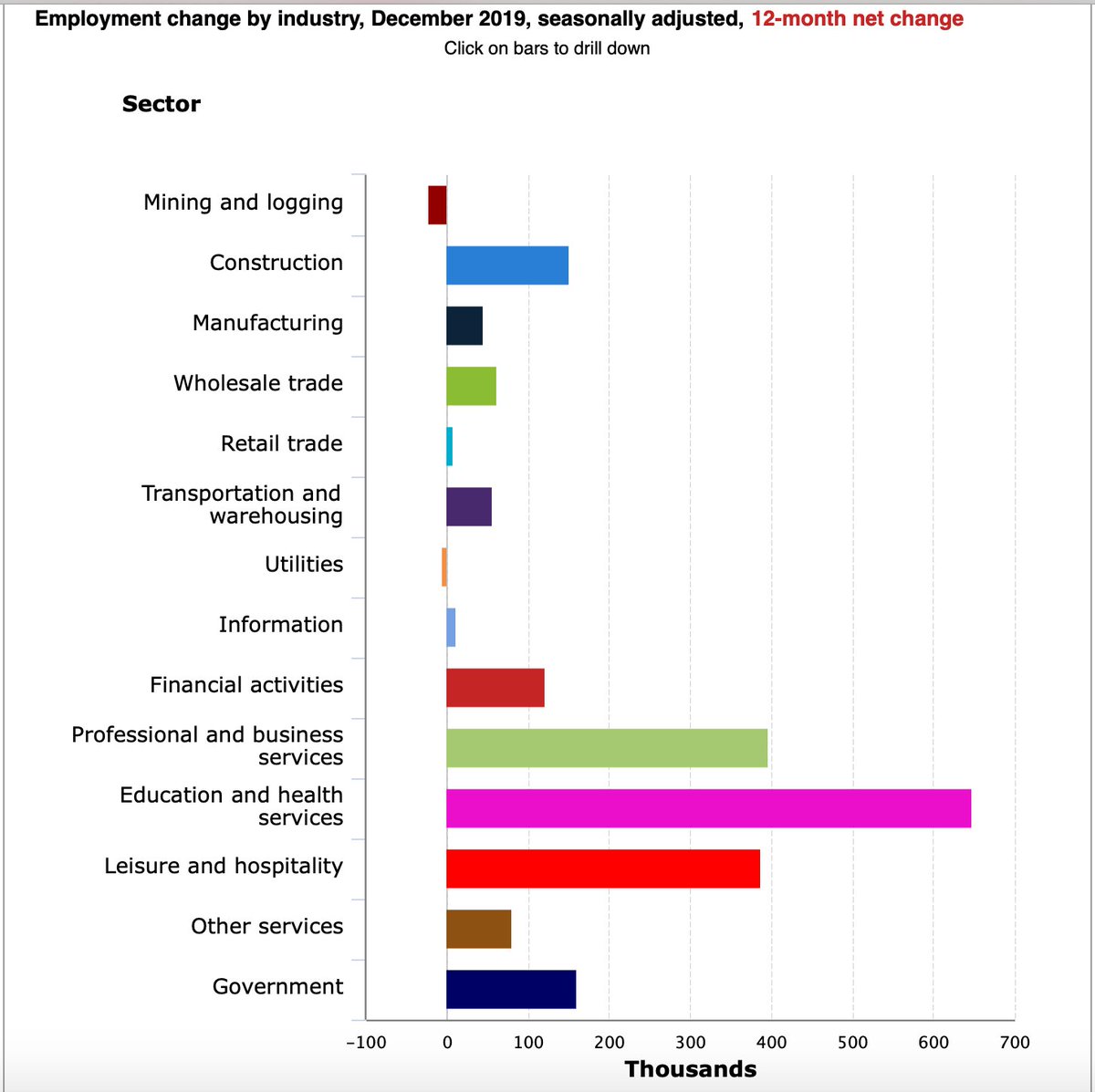
@BLS_gov 2. Since that time, the US has added ~1 million more #healthcare jobs, >50,000 more in 2019 than 2018. No sector grew more in 2019.
(NB Education + healthcare sum is ~90% healthcare related)
(NB Education + healthcare sum is ~90% healthcare related)

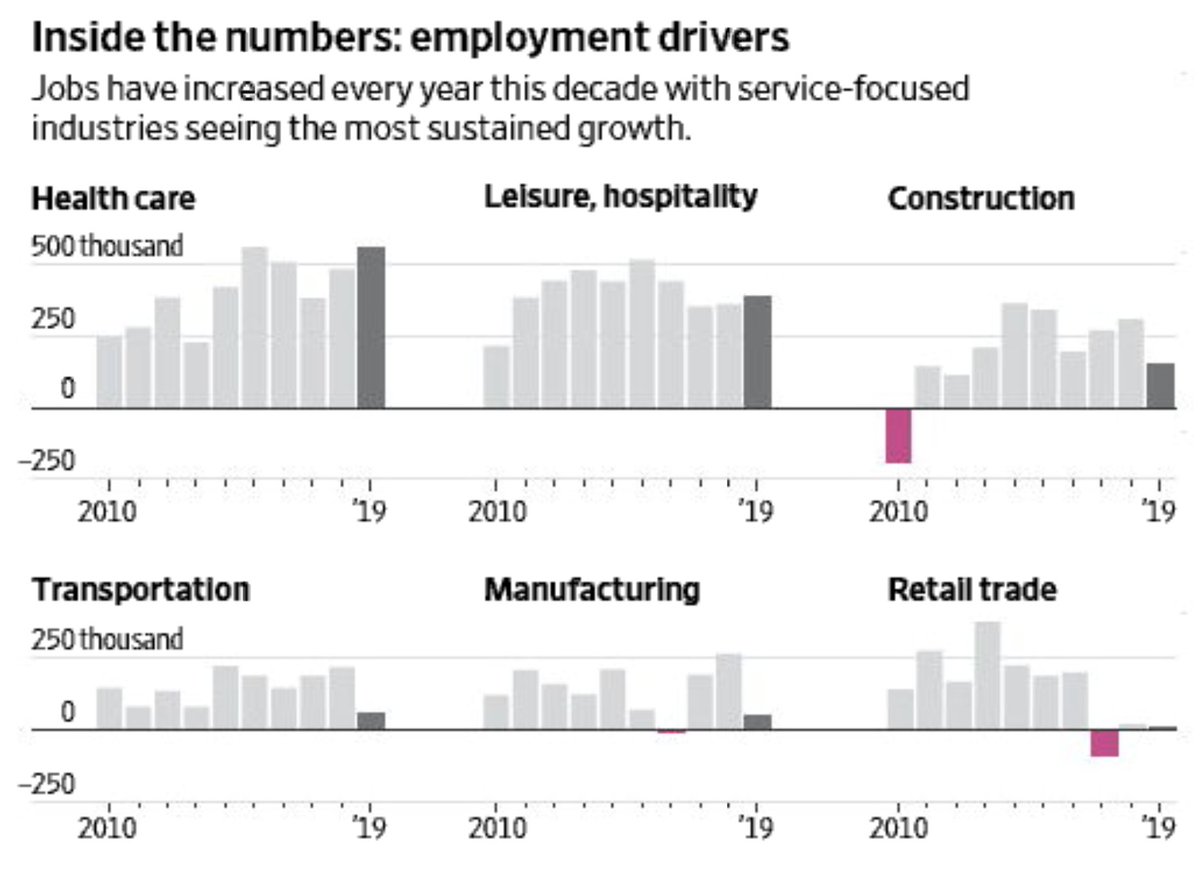
@BLS_gov 3. Healthcare added the most jobs throughout the past decade
wsj.com/articles/decem… by @EricMorath @TheAmaraReport
wsj.com/articles/decem… by @EricMorath @TheAmaraReport
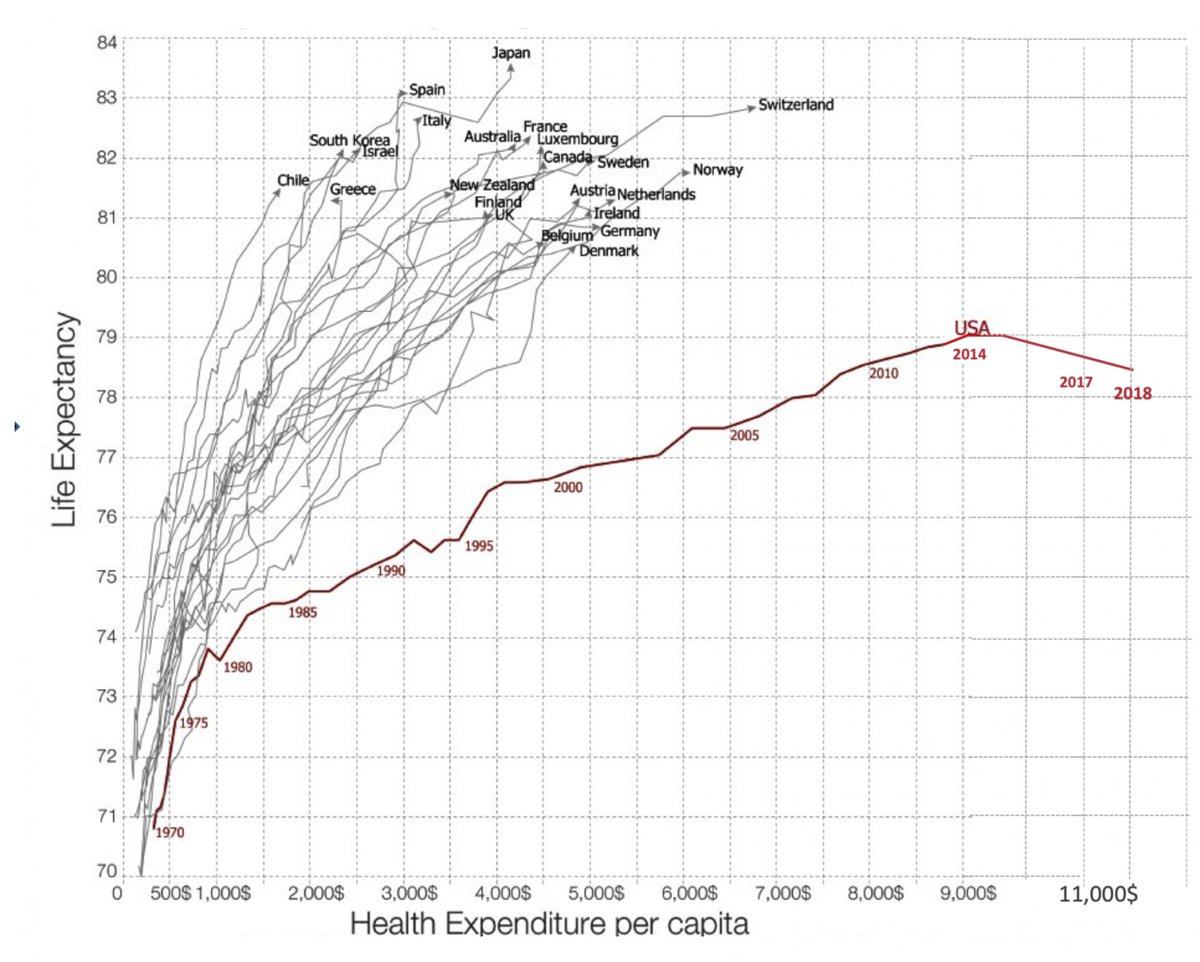
@BLS_gov @EricMorath @TheAmaraReport 4. Human capital, i.e. the workforce, is the #1 driver of costs of healthcare. In the US we now pay > $11,000 per person with the worst major outcomes of all 36 @OECD countries. There are no data to suggest that more labor support will improve outcomes.
growthevidence.com/growth-comment…
growthevidence.com/growth-comment…
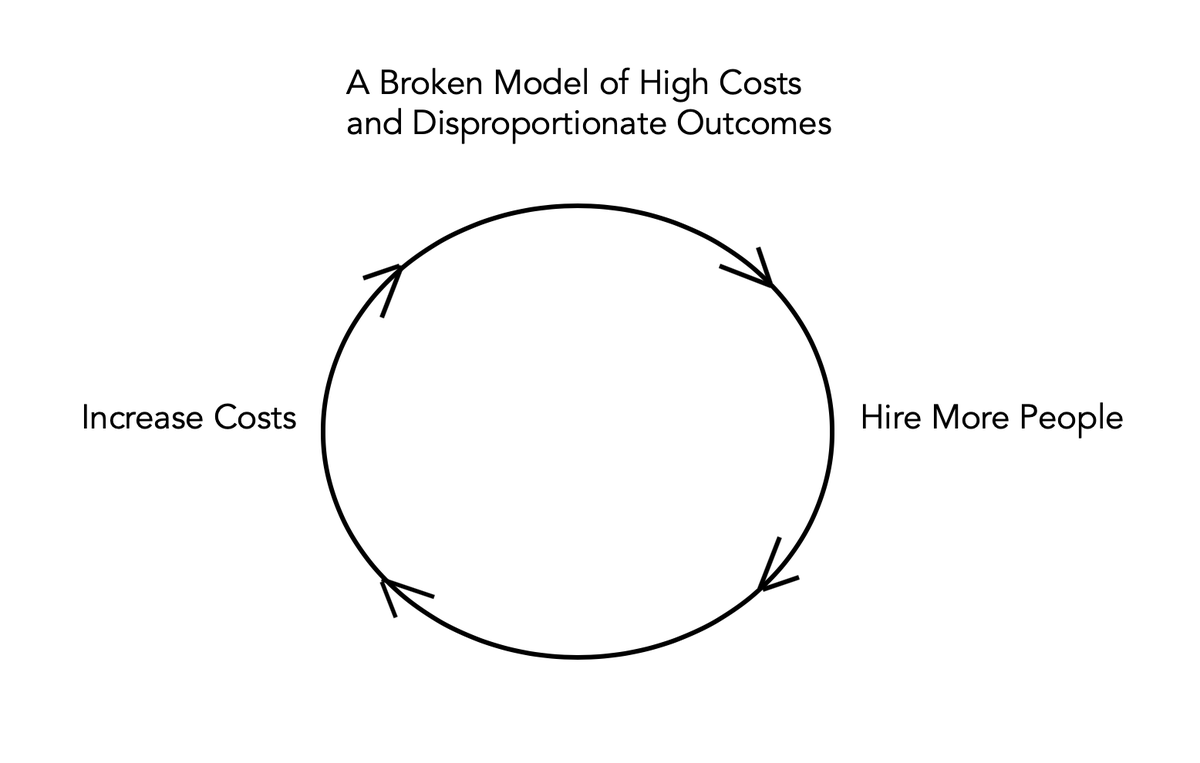
@BLS_gov @EricMorath @TheAmaraReport @OECD 5. So this is a feed the (broken) beast model. Nothing is being done to address it; the job growth is just celebrated.
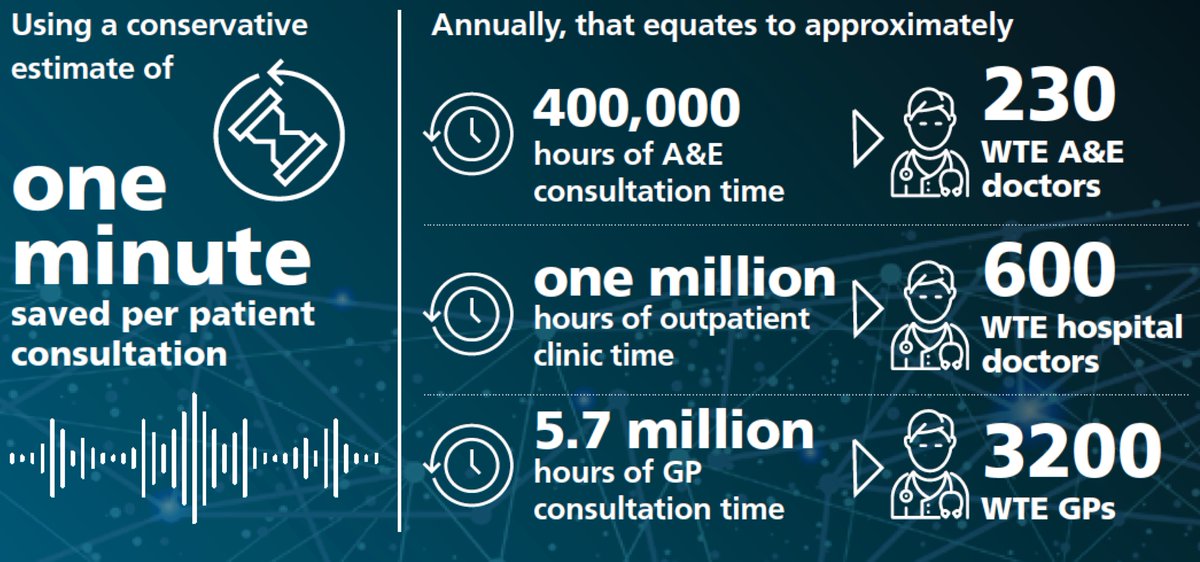
Whereas the UK (which has better outcomes at half the cost) undertook an in-depth review & is implementing many worthy strategies
topol.hee.nhs.uk
Whereas the UK (which has better outcomes at half the cost) undertook an in-depth review & is implementing many worthy strategies
topol.hee.nhs.uk
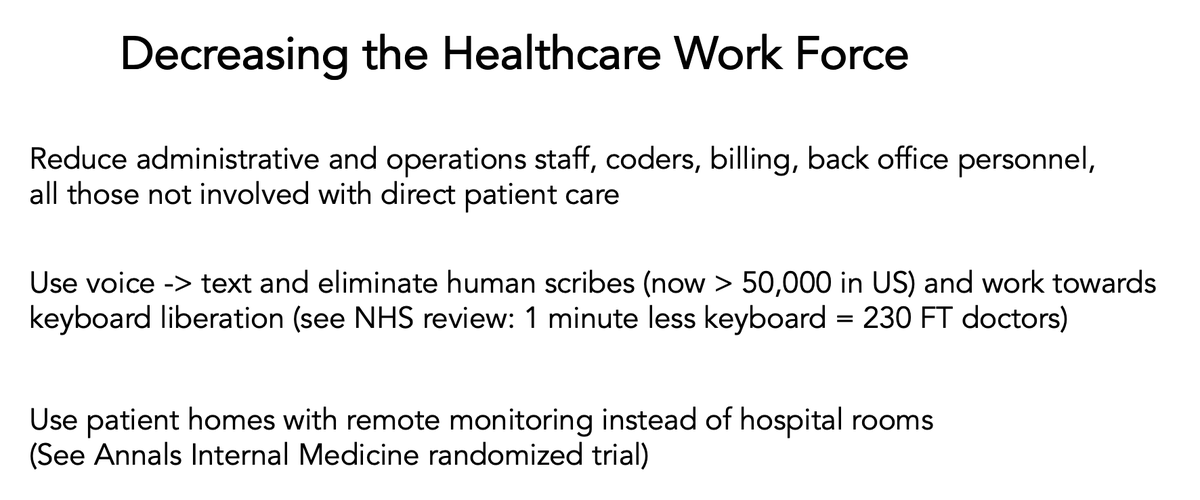
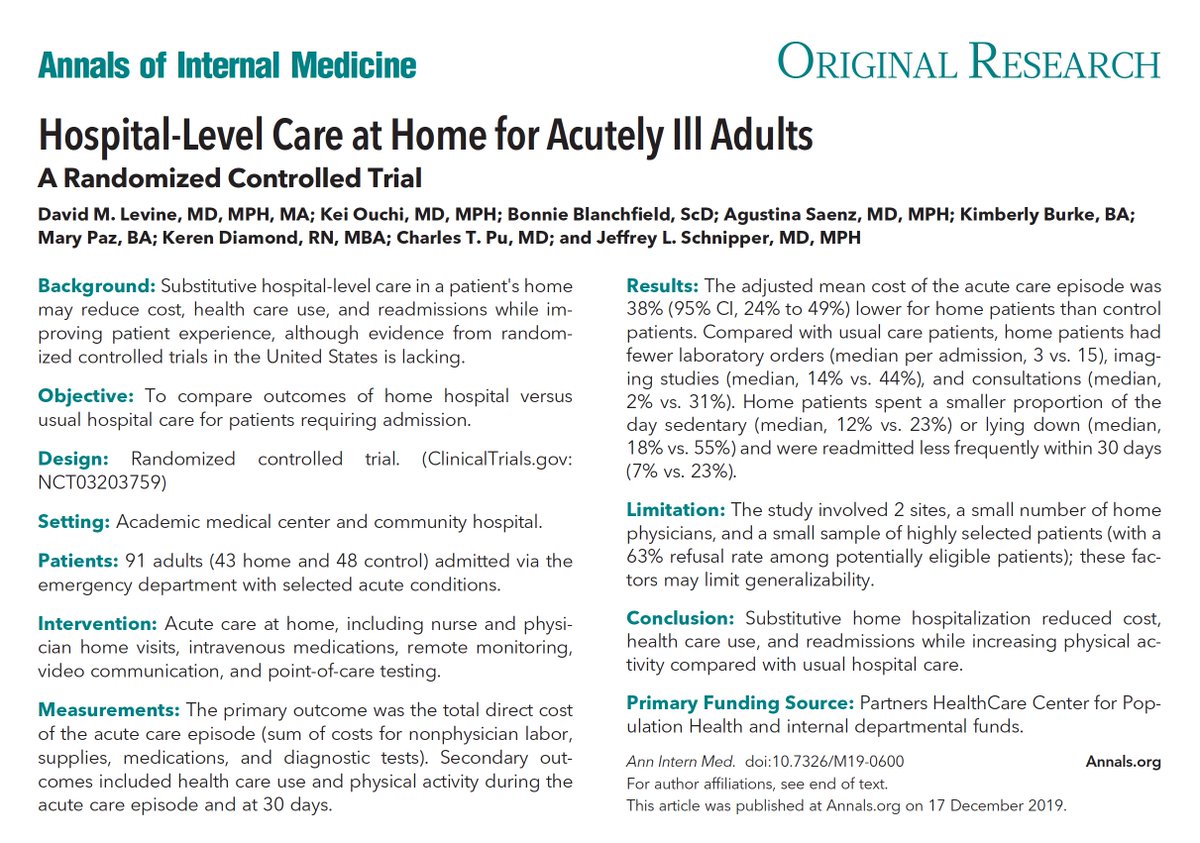
@BLS_gov @EricMorath @TheAmaraReport @OECD 6. To break up the vicious cycle, costs have to be lowered. Besides getting rid of administrative waste
(> $812,000,000,000 in 2017, annals.org/aim/fullarticl… @AnnalsofIM),
a reduction in the workforce can be accomplished.
(> $812,000,000,000 in 2017, annals.org/aim/fullarticl… @AnnalsofIM),
a reduction in the workforce can be accomplished.
• • •
Missing some Tweet in this thread? You can try to
force a refresh