
As promised, here is a ReCAP of my CE from this past week!
#FightTheBugs #SaveTheDrugs #TakeCareOfTheHumans #TwitteRx
#FightTheBugs #SaveTheDrugs #TakeCareOfTheHumans #TwitteRx

Pt presents w/ s/sx of CAP. First things first, let’s rule out flu. #DYK the guidelines prefer PCR over antigen assays? That’s because the antigen assays have a high risk of false negatives d/t low sensitivities. PCR=high sensitivity, can truly r/o viral infxn.

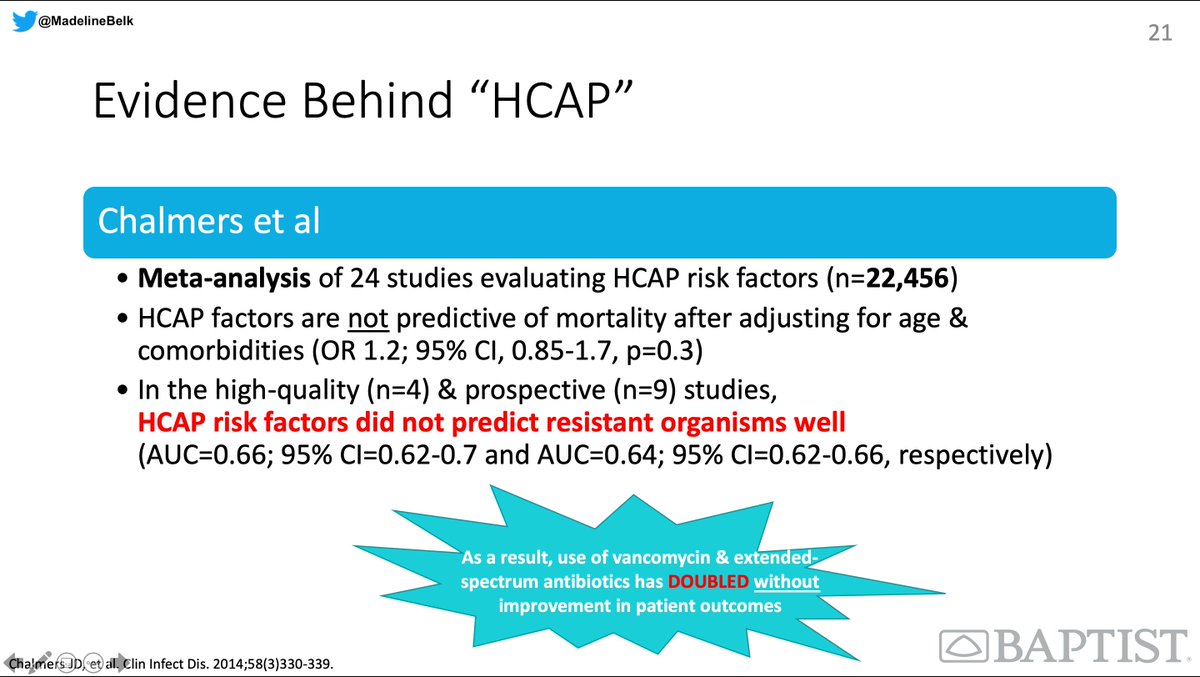
#Newsflash HCAP is no longer a thing! Chalmers et al conducted a meta-analysis of >20k:
👉🏼pts w/ HCAP risk factors weren’t an indicator for mortality or resistance pathogens
👉🏼pts classified as “HCAP” received double the amt of broad-spec abx w/ NO IMPROVEMENT in outcome‼️
👉🏼pts w/ HCAP risk factors weren’t an indicator for mortality or resistance pathogens
👉🏼pts classified as “HCAP” received double the amt of broad-spec abx w/ NO IMPROVEMENT in outcome‼️
The guidelines don't really help w/ determining who to cover w/ broad-spec abx though… not all hospitals have access to resources needed to determine these “locally validated risk factors” but luckily scoring systems have been developed to help out.

Main takeaway, cumulative risk factors > single risk factor. Among the top tools are the Shorr Score, which looks @ MDROs & is easy to conduct @ bedside (only 4 variables), & the Frei Score, which shows only high-risk pts have a mortality benefit when empirically covered for PsA.

Shorr et al also looked @ MRSA risk in CAP & found that the top risk factors were recent hospitalization & ICU admission. When pts have >/6 variables, their risk of MRSA infxn is ~30%.

2 steps forward, 3 steps back: that’s what happened w/ the updated GL’s rec on atypical coverage. But study conducted by Makabberi et al showed less treatment failures, better tolerance, and stat sign shorter LOS & lower cost to pts receiving doxy vs. FQ (PMID: 20456738).

Not “new” news but important nonetheless is macrolide duration. Azithromycin has wonderful tissue penetration & a long T1/2 that allows it to be given in a higher dose over a shorter period of time (3 days vs. 5 days). #TheMoreYouKnow

Guess what!? Standard CAP-treatment recommendations already have anaerobic coverage! When do you need more you ask?
Two cases:
☝️🏼empyema
✌️🏼abscess
Note: NOT aspiration PNA, I repeat, NOT aspiration PNA.
Two cases:
☝️🏼empyema
✌️🏼abscess
Note: NOT aspiration PNA, I repeat, NOT aspiration PNA.

Let’s emphasize & embrace that less really is more. Study by Uranga et al showed 5 days to be noninferor to 10 days for CAP tx. Some cases may require longer durations (L. pneumophila, Mycobacterium tuberculosis, etc.) but for most pts 5 days is adequate.

#IMO The best thing about the changes is the overhaul of HCAP. Each pt should be individually assessed for MDRO risk, remembering that cumulative risk factors mean a lot more than a single risk factor (unless, of course, that risk is prior hx of MDRO!) #ThanksForFollowingAlong 🤓

• • •
Missing some Tweet in this thread? You can try to
force a refresh


