
"Cytokine Storm". The idiot's buzzword of the week. It makes you sound smarter if you say it often enough. When I first heard of it in 1994 it sounded AMAZING! Then this RCT came out showing it increased mortality. Ouch nejm.org/doi/full/10.10…
Next came rhAPC (drotrecogin). Don't knock out the immune system: we need it to survive. APC has signalling properties to modulate inflammation. NEJM PROWESS was touted a success! nejm.org/doi/full/10.10…
Just as we were celebrating and retrospective analyses showed efficacy correlated with drotrecogin reducing Il-6 levels, bad news came in and the dream turned sour nejm.org/doi/full/10.10…
These treatments looks so promising in animals models, in phase 1, 2 & even 3 trials. All to no avail. For some, like me, the dream lives on! One day the right modulatory agent will be found. But IL-6 inhibitors are too crude a therapy jamanetwork.com/journals/jama/…
We are facing a crisis from a virus against which we have no proven treatments. Repeating the phrase "cytokine storm" as your infinite mantra as you resort to cavalier adventurism out of sheer panic violates the principle of DO NO HARM #CytokineStorm #COVID4MDs #FOAMcovid
These treatments looked so promising in animals models, in phase 1, 2 & 3 trials. All to no avail. For some, like me, the dream lives on! One day the right modulatory agent will be found. But IL-6 inhibitors are too crude a therapy jamanetwork.com/journals/jama/…
We are facing a crisis from a virus against which we have no proven treatments. Repeating the phrase "cytokine storm" as your infinite mantra as you resort to cavalier adventurism out of sheer panic violates the principle of DO NO HARM #CytokineStorm #COVID4MDs #FOAMcovid
I really do want to see progress with immuno(thrombo)modulation of sepsis/SIRS but it's seen so many setbacks. I can list many promising avenues for the future. But rash experimentation risks bringing it more into disrepute if it increases mortality. We don't want that #COVID4MDs
Another caveat. Historically, immuno(thrombo)modulation of a decompensated immune response = 2nd line therapy after failure to respond to appropriate antibiotic treatment. Immunosuppression without any effective antiviral treatment is a whole new ballgame #COVID4MDs
@nature publishes misgivings similar to my own about the rush to treat COVID-19 with immunosuppressants. Using the term "cytokine STORM" as a call to action instead of "cytokine release syndrome" is another problem nature.com/articles/d4158… #COVID4MDs
That Nature article failed to give sufficient warning about the potential dangers of steroids for #COVIF19. This Lancet article argues that steroids should only be given as part of an RCT
My next objection to a mad rush to immunosuppress after declaring the immune system public enemy number 1. There is lymphopoenia in COVID-19 as in HIV. Are we already too immunosuppressed?
Another objection to Il-6 blockers. We scream the "cytokine storm" mantra, meaning that an immune response is good but too much of a good thing is bad. Doesn't that mean we want to reduce excess Il-6 down to an ideal therapeutic range? Who checks Il-6 levels before and after Rx?
The truth is that nobody has done a large animal COVID-19 dose titration study to find what the optimal Il-6 level is in sepsis, let alone a Phase I clinical trial in humans. You just assume Il-6 = BAD. Ergo knock it out completely, the lower the Il-6 level the better. Why?
Next possible issue with Il-6 inhibitors. More men die from COVID-19 than women. TLR7 is inherited on the X chromosome. Women transcribe from both copies of the gene resulting in macrophages, NK cells, dendritic cells, lymphocytes expressing more TLR7 immunology.sciencemag.org/content/3/19/e…
TLR7 allows the innate immune system to recognise single-stranded RNA viruses like SARS-COV-2. If women express twice as much TLR7 than men this may result in more efficient viral clearance, improving outcomes cell.com/pb-assets/prod… 
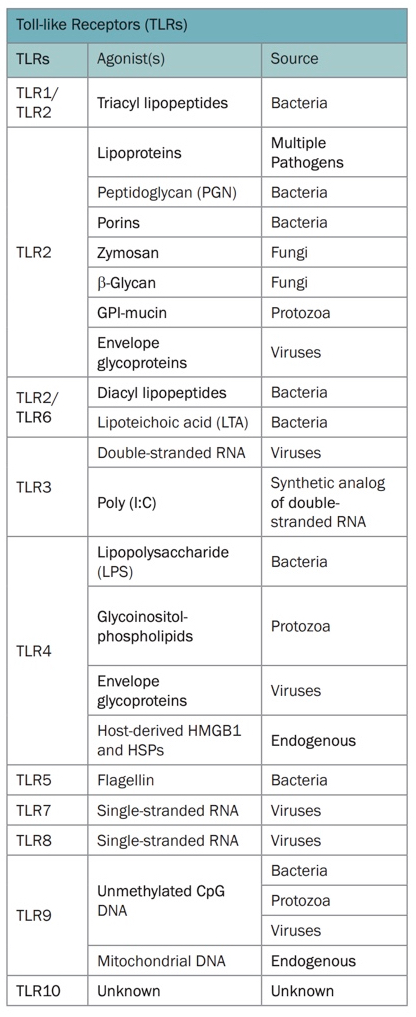
But TLR7 also drives the output of Il-6. ncbi.nlm.nih.gov/pmc/articles/P… The reason for the lower mortality from COVID-6 in women might be due to a brisker TLR7 mediated Il-6 immune response. Il-6 might be the fire engine rather than the fire storm.
Advocates of Il-6 blockade are touting this retrospective subgroup analysis years later of Il-1 blockade as evidence of the success of immunomodulatory therapy. But such subgroup analyses are prone to bias and the authors recommend an RCT ncbi.nlm.nih.gov/pmc/articles/P…
Here is the original RCT of Il-1 blockade in sepsis. It was a negative trial: "rhIL-1ra failed to demonstrate a statistically significant reduction in mortality when compared with standard therapy in this multicenter clinical trial" ncbi.nlm.nih.gov/pubmed/9233735
Such Il-1R blockade trials were again NOT trials of its usage as a substitute for antimicrobial therapy. Il-6 COVID trials like the following don't even target specific subgroups proven to have macrophage activation syndrome (or severely elevated Il-6 etc) medrxiv.org/content/10.110…
Another uncontrolled trial of Il-6R blockade with Tocilizumab that doesn't serologically demonstrate macrophage activation syndrome (or similar elevation in Il-6 etc) before starting it as an ersatz antiviral drug medrxiv.org/content/10.110…
The Tocilizumab for COVID-19 trial begs the question of why an immunosuppressive drug known to cause serious viral infections is being used as an ersatz antiviral drug. See for eg this report of CMV pneumonitis in a rheumatoid arthritis patient ncbi.nlm.nih.gov/pmc/articles/P…
One paper dismisses risks of worsening COIVD-19: "IL-6 blockade results in reduction of IL-10, an immunosuppressive cytokine... which may mitigate concerns about prolonging viral clearance". But no clinical/animal studies exist to support this in COVID-19 science.sciencemag.org/content/early/…
The above authors then allege "one or two doses of an IL-6 antagonist are unlikely to result in fungal infections which occur in patients dosed monthly for conditions such as rheumatoid arthritis". How can they guarantee this in ICU patients on ventilators for weeks?

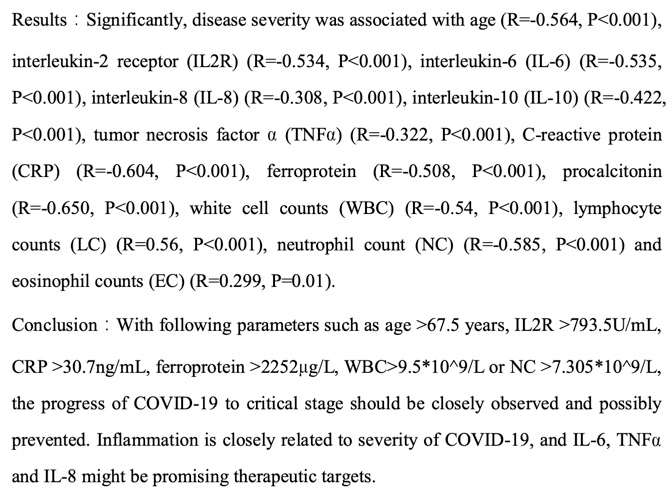
To counter my grave concerns, people quote studies like this at me showing correlations between outcomes & Il-6 levels. Next they want to knock out Il-2/6/8/TNFa etc as if chanting the "cytokine storm" mantra magically transformed it into a cure medrxiv.org/content/10.110…
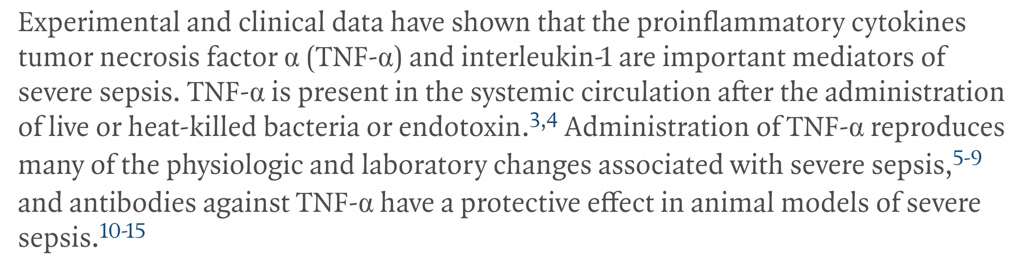
But none of this is new. Let's return to the NEJM TNFa inhibitor trial that worsened mortality in sepsis. This is what killed off the 1990s approach of knocking different cytokines in the hope of finding a "cure" but a new generation has forgotten this nejm.org/doi/full/10.10…
Some complain that labelling the "cytokine storm" concept an idiot's mantra is too brutal. As Alexander Pope wrote in 1711 "fools rush in where angels fear to tread". I have a duty to issue grave warnings where there is fair concern for patient safety. Only a fool disregards that
For in 1711 Pope also said: "A little learning is a dang'rous thing". Those chanting the infinite mantra of the "cytokine storm" ignore the grave lessons of the past. As Andre Kalil says: “Many drugs we believed were fantastic ended up killing people” nytimes.com/2020/04/09/hea…
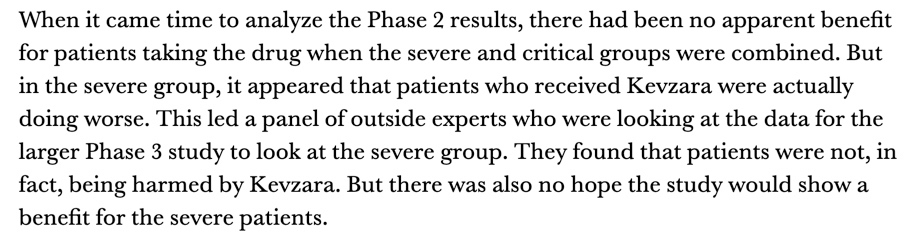
And there we have it, before I could add another tweet to the thread. Data suggesting a trend towards harm tricking in for Il-6R blocker, Sarilumab. RCT terminated statnews.com/2020/04/27/art…
Even Regeneron and Sanofi admit that giving Il-6R inhibitors for COVID-19 is a "kitchen sink" (sic) approach to treatment statnews.com/2020/04/27/art…
A problem with the Il-6RA trials is that pharma companies have been too keen to rebrand their drug as a cure-all for COVID-19 instead of selecting subgroups with macrophage activation syndrome & Il-6 elevations into CAR T cell CRS levels.
When you do the groundwork it turns out the cellular and molecular response patterns in COVID-19 are totally unlike CAR T cell CRS. This should have been checked before starting clinical trials instead of making assumptions about them being the same
Note the same authors hypothesise that CV19 may deploy an immune evasion strategy. We know too little about the immune response to CV19 to be able to leap to the fatal conclusion that immune hyperresponsiveness suffices to explain all ills

