0/ Buongiorno, #medtwitter! We bring to you a #tweetorial on ventilator management for all those folks who don’t normally manage ARDS who have stepped up to help in this pandemic.
All credit goes to @AvrahamCooperMD; the following tweetorial is his brainchild. Thanks, Avi!
All credit goes to @AvrahamCooperMD; the following tweetorial is his brainchild. Thanks, Avi!
1/ Many clinicians are being/will be called to manage ARDS on the ventilator.
Imagine that your patient has just been intubated. Let's walk through the steps of vent mgmt 101:
- Initial housekeeping
- Basic vent management decisions in ARDS
- Management of refractory hypoxemia
Imagine that your patient has just been intubated. Let's walk through the steps of vent mgmt 101:
- Initial housekeeping
- Basic vent management decisions in ARDS
- Management of refractory hypoxemia

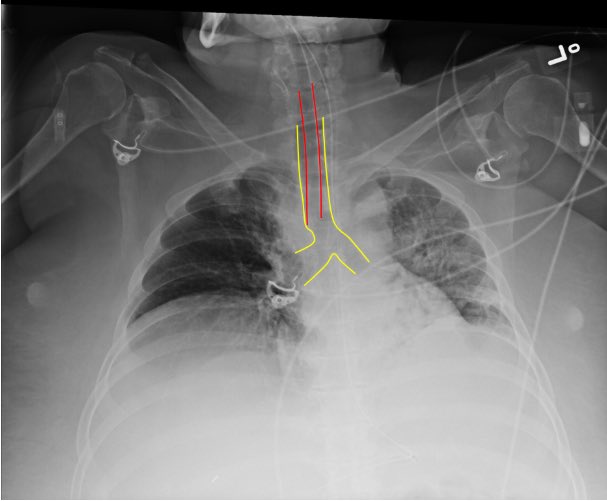
2/ First, confirm endotracheal tube position:
- Did capnography confirm tracheal placement?
- Are breath sounds bilateral?
- Is the tube placed appropriately on CXR? (typically 2-5 cm from carina)
Pic from SAEM bit.ly/3bJrTpa
- Did capnography confirm tracheal placement?
- Are breath sounds bilateral?
- Is the tube placed appropriately on CXR? (typically 2-5 cm from carina)
Pic from SAEM bit.ly/3bJrTpa
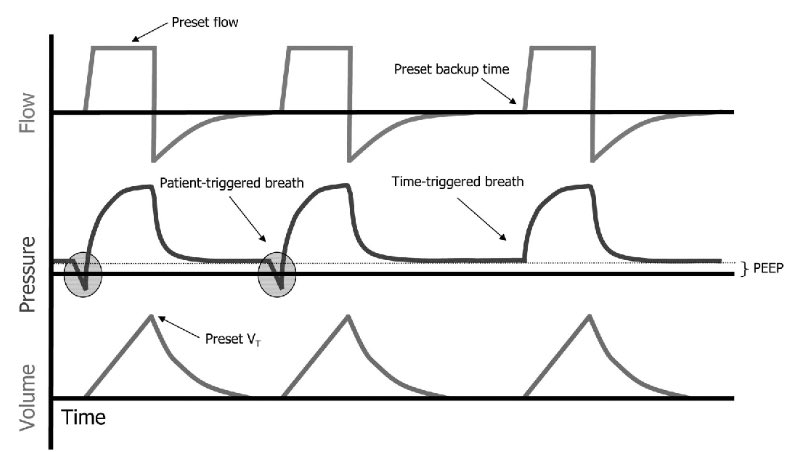
3/ Next, set the ventilator. You'll need to choose an initial setting.
Typically this will be assist control/volume control (AC/VC) which allows you to:
✔️ Maintain low tidal volume ventilation
✔️ Guarantee a respiratory rate
Pic from bit.ly/3462mny
Typically this will be assist control/volume control (AC/VC) which allows you to:
✔️ Maintain low tidal volume ventilation
✔️ Guarantee a respiratory rate
Pic from bit.ly/3462mny
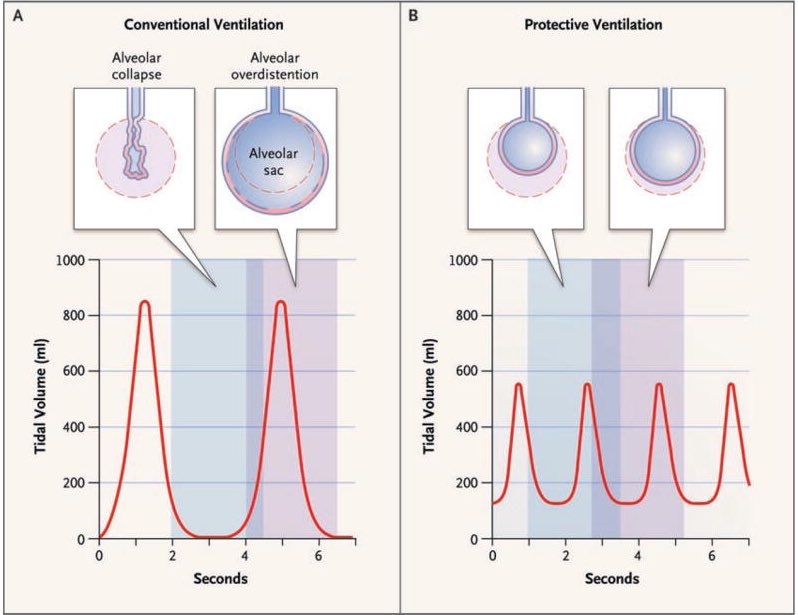
4/ You'll need to set minute ventilation (MV = tidal volume x respiratory rate)
-Try to approximate pre-intubation MV (not always possible)
-Use low tidal volume ventilation (4-8 ml/kg ideal body weight)
-Goal plateau pressure < 30 mmHg
-Goal pH > 7.2
ncbi.nlm.nih.gov/pubmed/17855672
-Try to approximate pre-intubation MV (not always possible)
-Use low tidal volume ventilation (4-8 ml/kg ideal body weight)
-Goal plateau pressure < 30 mmHg
-Goal pH > 7.2
ncbi.nlm.nih.gov/pubmed/17855672
5/ Finally, set PEEP/FiO2:
- Avoid O2 sats of 100% (hyperoxia is bad), aim for 92%-95%
- Set adequate PEEP, typically >10 mmHg in ARDS
COVID19 patients are PEEP-sensitive. In general aim for higher PEEP and lower FiO2.
ebmedicine.net/topics/infecti…
- Avoid O2 sats of 100% (hyperoxia is bad), aim for 92%-95%
- Set adequate PEEP, typically >10 mmHg in ARDS
COVID19 patients are PEEP-sensitive. In general aim for higher PEEP and lower FiO2.
ebmedicine.net/topics/infecti…
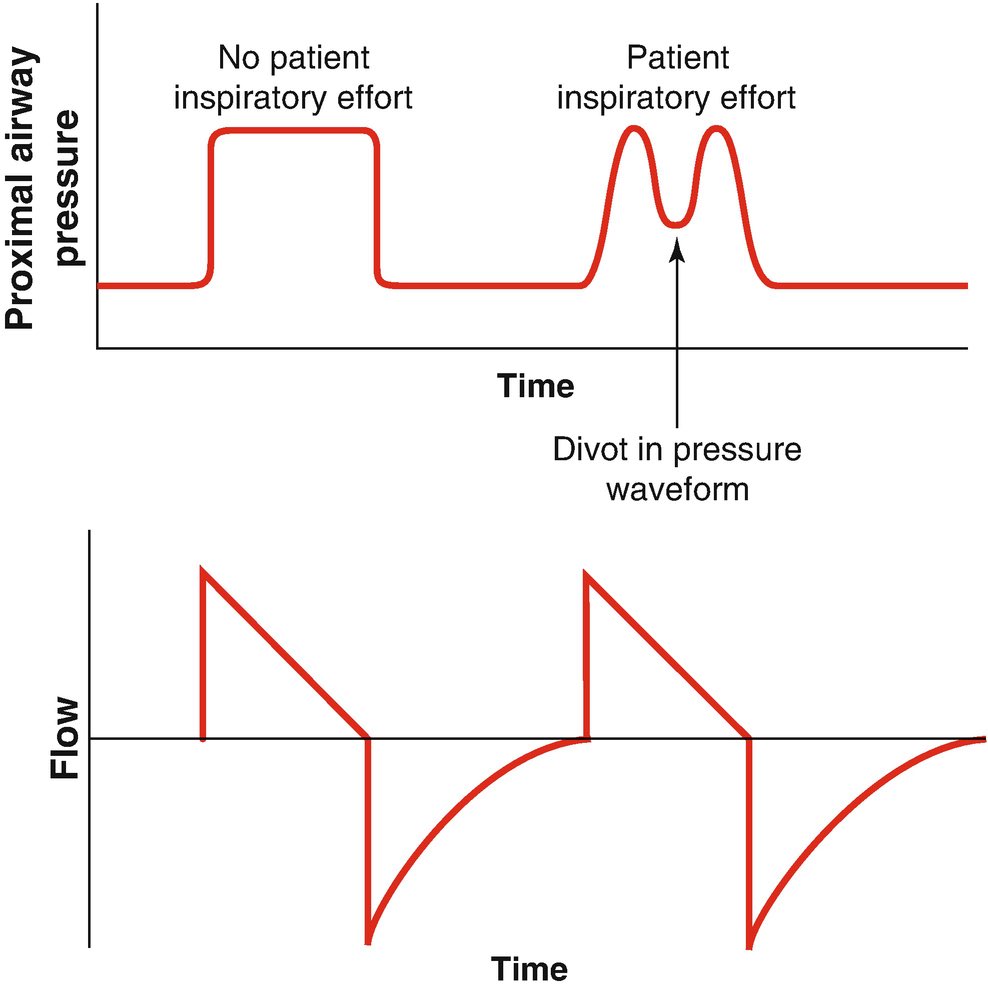
6/ Now that the ventilator's set, choose a sedation strategy.
- Patients with moderate to severe ARDS usually need sedation to ensure vent synchrony
- Vent Dyssynchrony ⬇️ oxygenation and ⬆️ lung injury
- Whatever sedation you choose, achieve synchrony
link.springer.com/chapter/10.100…
- Patients with moderate to severe ARDS usually need sedation to ensure vent synchrony
- Vent Dyssynchrony ⬇️ oxygenation and ⬆️ lung injury
- Whatever sedation you choose, achieve synchrony
link.springer.com/chapter/10.100…
7/ Some patients will oxygenate well with adequate PEEP and sedation.
Others will require additional therapies. Let's briefly review:
😑Paralysis
🙃Proning
😮Inhaled pulmonary vasodilators
Others will require additional therapies. Let's briefly review:
😑Paralysis
🙃Proning
😮Inhaled pulmonary vasodilators
8/Who may require paralysis?
Those patients that remain dyssynchronous/hypoxemic despite sedation.
Paralysis does not improve mortality in severe ARDS but individual patients may benefit.
nejm.org/doi/full/10.10…
Those patients that remain dyssynchronous/hypoxemic despite sedation.
Paralysis does not improve mortality in severe ARDS but individual patients may benefit.
nejm.org/doi/full/10.10…
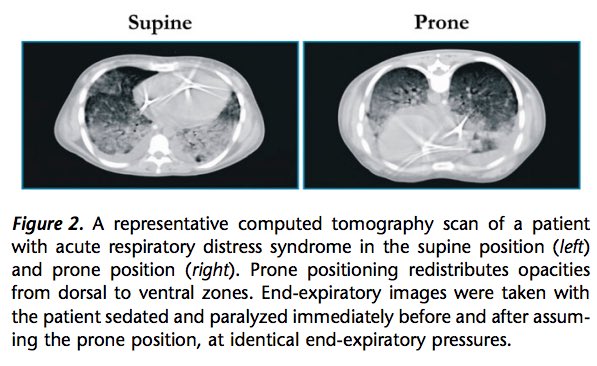
9/ Benefits of proning?
✔️Turning patients to the prone position optimizes V/Q matching and lung recruitment, and may dramatically improve hypoxemia.
✔️It has been shown to reduce mortality in those with PaO2:FiO2 < 150.
ncbi.nlm.nih.gov/pubmed/24134414
✔️Turning patients to the prone position optimizes V/Q matching and lung recruitment, and may dramatically improve hypoxemia.
✔️It has been shown to reduce mortality in those with PaO2:FiO2 < 150.
ncbi.nlm.nih.gov/pubmed/24134414
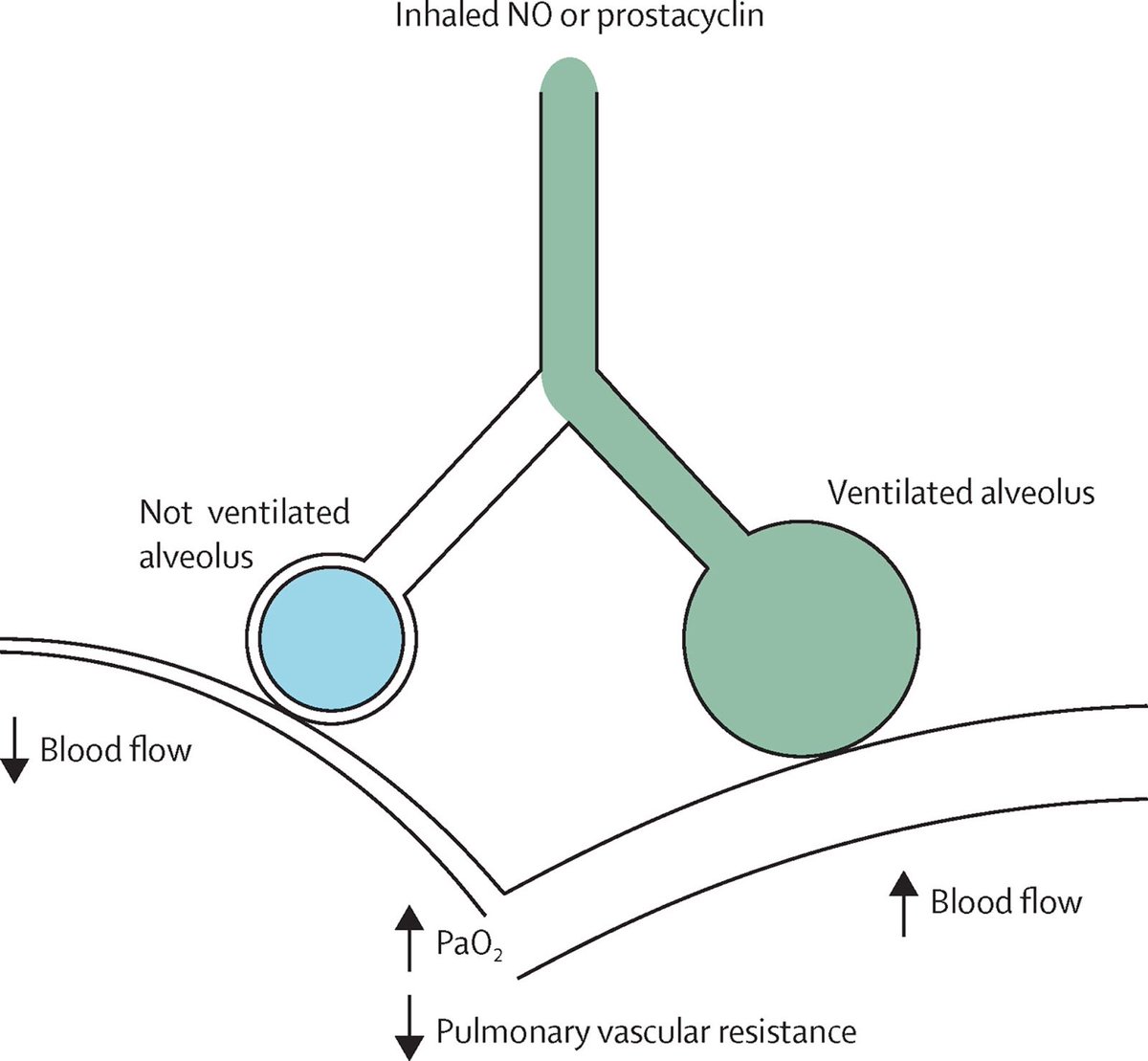
10/ What are ex. of inhaled pulmonary vasodilators?
1️⃣Epoprostenol or
2️⃣nitric oxide
- Preferentially vasodilate aerated lung units, ⬆️ V/Q matching and ⬆️ SpO2
- No impact on mortality or lung mechanics so should only be added for refractory hypoxemia
ncbi.nlm.nih.gov/pubmed/27203510
1️⃣Epoprostenol or
2️⃣nitric oxide
- Preferentially vasodilate aerated lung units, ⬆️ V/Q matching and ⬆️ SpO2
- No impact on mortality or lung mechanics so should only be added for refractory hypoxemia
ncbi.nlm.nih.gov/pubmed/27203510
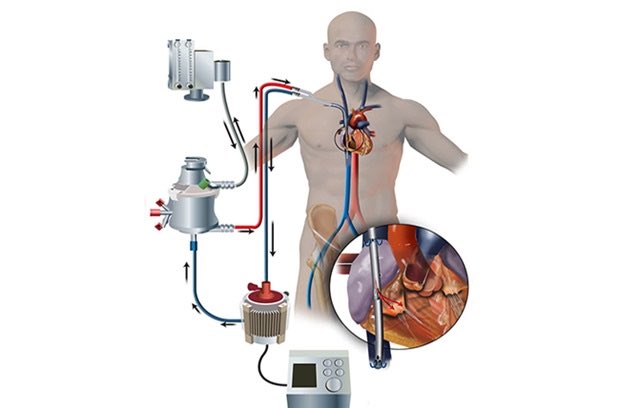
11/ Finally, when to call the veno-venous ECMO team.
There's no hard/fast rule but this is reserved for patients w/ refractory severe hypoxemia or respiratory acidosis despite conventional therapies.
A general rule is "it's better to call for ECMO too early than too late."
There's no hard/fast rule but this is reserved for patients w/ refractory severe hypoxemia or respiratory acidosis despite conventional therapies.
A general rule is "it's better to call for ECMO too early than too late."
12/ To summarize:
✔️ Confirm tube position
✔️Low tidal volumes, adequate PEEP
✔️Tolerate respiratory acidosis
✔️ Sedate for synchrony
✔️ If still hypoxemic, prone and probably paralyze, inhaled vasodilators if refractory
✔️ Better to call for ECMO too early than too late
✔️ Confirm tube position
✔️Low tidal volumes, adequate PEEP
✔️Tolerate respiratory acidosis
✔️ Sedate for synchrony
✔️ If still hypoxemic, prone and probably paralyze, inhaled vasodilators if refractory
✔️ Better to call for ECMO too early than too late