
Need a quick recap on #AirwayManagement for nonintensivist? EP: 206 @thecurbsiders @chungk1031 @DoctorWatto @PaulNWilliamz @BrighamSK @Askins_Razor
Breathe easy w/ these airway management principles & expert tips for managing the pt w/ COVID-19 related lung disease
Part 1 of 2
Breathe easy w/ these airway management principles & expert tips for managing the pt w/ COVID-19 related lung disease
Part 1 of 2
Airway Management Pearls
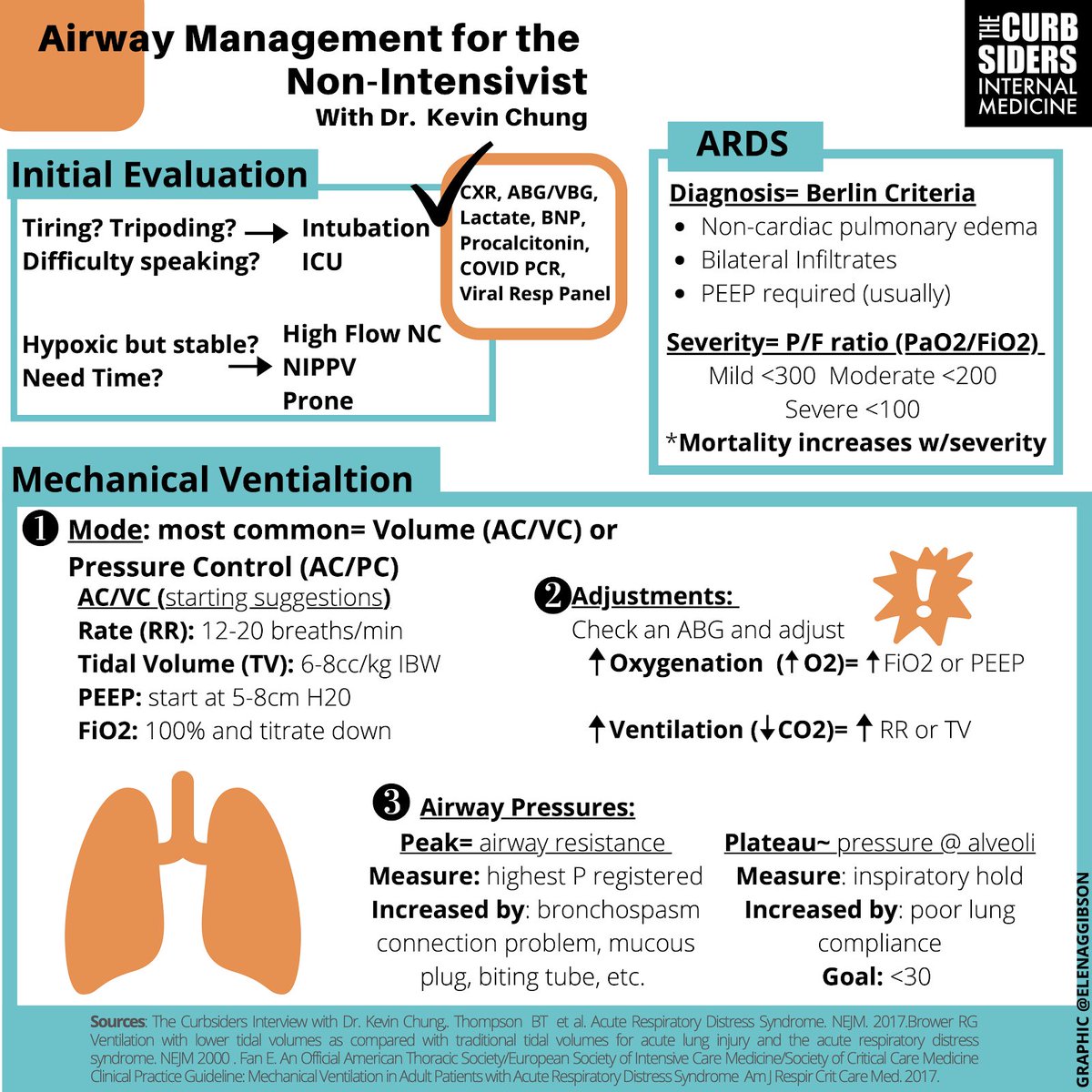
1. High flow nasal cannula (HFNC): Start at 10-20 LPM and 100% FIO2 and ask patients to breathe in through their nose, out through their mouth and purse their lips to generate PEEP.
1. High flow nasal cannula (HFNC): Start at 10-20 LPM and 100% FIO2 and ask patients to breathe in through their nose, out through their mouth and purse their lips to generate PEEP.
2. In general, basic mechanical ventilation can be thought of us in terms of volume assist control and pressure assist control – the former being more common/intuitive, where a tidal volume is set versus the latter where expiratory and inspiratory pressures are set.
3. In volume control assist ventilation (AC/VC): fraction of inspired oxygen (FiO2) and positive end-expiratory pressure (PEEP) can be adjusted to improve oxygenation while respiratory rate (RR) and tidal volume (VT) can be adjusted to improve ventilation.
4. Keep an eye on peak and plateau pressures: elevations in one or both have a differential diagnosis (see below) which can guide troubleshooting efforts.
5. Compliance refers to how easily the lung distends – this should be regularly assessed (by plateau pressure)
5. Compliance refers to how easily the lung distends – this should be regularly assessed (by plateau pressure)
6. Ventilator Dyssynchrony rarely means the patient is suffering from a sedation deficiency: consider making adjustments to the ventilator, including flow or trying a different ventilator mode. When in doubt, call your friendly neighborhood intensivist for help.
7. ARDS is defined via the Berlin Criteria and graded in severity using the P:F ratio. Proning, paralyzing, optimizing PEEP and pruning (diuresing) are strategies to help patients with advanced ARDS.
Initial Patient Contact & Assessment:
In the context of the current COVID-19 pandemic, hypoxemia w/ bilateral CXR findings upon presentation is concerning.
Dont stop being a good internist! Consider a broad differential.
Hx of heart disease?
Hx of CHF?
Other viral illnesses?
In the context of the current COVID-19 pandemic, hypoxemia w/ bilateral CXR findings upon presentation is concerning.
Dont stop being a good internist! Consider a broad differential.
Hx of heart disease?
Hx of CHF?
Other viral illnesses?
Physical Exam:
Be quick! Make note of accessory muscle use.
Listen for evidence of murmur, perhaps a quick lung exam – make sure to use proper PPE!
Be quick! Make note of accessory muscle use.
Listen for evidence of murmur, perhaps a quick lung exam – make sure to use proper PPE!
Labs: ABG (or VBG) with lactate, brain natriuretic peptide (BNP), procalcitonin, respiratory viral PCR panel, COVID-19 PCR (keeping in mind the specificity > sensitivity.
Dr. Watto pointed out – consider getting two or even three in patients with a high pretest probability).
Dr. Watto pointed out – consider getting two or even three in patients with a high pretest probability).
Procalcitonin: very high procalcitonin can suggest a bacterial process which is either the primary pathology or may suggest coinfection .
Kashlak Pearl!: the coronavirus tested for on the respiratory viral PCR panel is not the novel coronavirus
Kashlak Pearl!: the coronavirus tested for on the respiratory viral PCR panel is not the novel coronavirus
Disposition:
These patients should be strongly considered for admission, close monitoring w/ continuous pulse oximetry, & supplemental O2 should be provided as needed.
Would further consider admission to the ICU, especially if NC O2 needs on admission are greater than > 6LPM
These patients should be strongly considered for admission, close monitoring w/ continuous pulse oximetry, & supplemental O2 should be provided as needed.
Would further consider admission to the ICU, especially if NC O2 needs on admission are greater than > 6LPM

