(THREAD) I teach communications and journalism at the university level. My published curatorial journalism relies exclusively on information from experts. Right now our medical experts are confusing America on some basic COVID-19 points. I'm going to try to help. Please RETWEET. 

1/ Right now we have two major, ongoing communications and journalism issues in the United States:
1⃣ Media is covering proclamations by non-experts on subjects that require expertise to discuss cogently.
2⃣ Experts are not using fully briefed intermediaries to deal with media.
1⃣ Media is covering proclamations by non-experts on subjects that require expertise to discuss cogently.
2⃣ Experts are not using fully briefed intermediaries to deal with media.
2/ The result is that when we turn on our TVs, either we're hearing from people we shouldn't be hearing from at all—individuals speaking way outside their areas of expertise (if they even have any)—*or* we are hearing *directly* from experts *who don't have communication skills*.
3/ The result of this situation is that Americans are getting misinformed *intentionally* when they hear from non-experts and misinformed *accidentally* when they hear from experts. So *no one* is operating in a communications network that feels *safe, reliable, and instructive*.
4/ Here are a few key COVID-19 facts that hard-working, well-intended medical experts without much in the way of communication skills have managed to—sometimes despite themselves—communicate to information-starved Americans:
1⃣ "Daily new deaths" is "lagging indicator."
[cont.]
1⃣ "Daily new deaths" is "lagging indicator."
[cont.]
5/
2⃣ This means that the confirmed daily death toll from COVID-19 nationally reflects infections that occurred *some time ago*, because COVID-19 takes a fairly long while to run its course from infection to "case closure" via either recovery or (God forbid) the patient's death.
2⃣ This means that the confirmed daily death toll from COVID-19 nationally reflects infections that occurred *some time ago*, because COVID-19 takes a fairly long while to run its course from infection to "case closure" via either recovery or (God forbid) the patient's death.
6/
3⃣ For cases that result in death, the average time from infection to death—usually as the patient is breathing on a ventilator in a hospital—is 18.5 days.
4⃣ This encourages the view that daily death toll spikes approximately 17 to 20 days after we see a spike in infections.
3⃣ For cases that result in death, the average time from infection to death—usually as the patient is breathing on a ventilator in a hospital—is 18.5 days.
4⃣ This encourages the view that daily death toll spikes approximately 17 to 20 days after we see a spike in infections.
7/
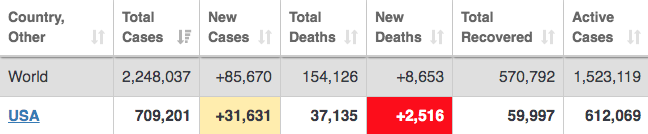
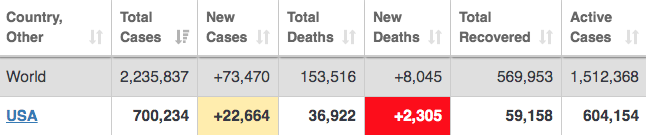
5⃣ So far, this "lagging indicator" maxim has proven to be accurate—per published data—at least 3 times, with the third death-toll spike possibly coming today (America has 2,305 deaths as of 6PM EST). This is a reflection of a spike in confirmed infections 17 to 20 days ago.
5⃣ So far, this "lagging indicator" maxim has proven to be accurate—per published data—at least 3 times, with the third death-toll spike possibly coming today (America has 2,305 deaths as of 6PM EST). This is a reflection of a spike in confirmed infections 17 to 20 days ago.
8/ Originally, researchers used data from China to model what might happen in the U.S. with respect COVID-19 mortality rates. We've since learned that there is reason to doubt the accuracy of the data coming out of China. So Italy, instead, became a much better model for America.
9/ What the data from Italy showed us is that *even with draconian social distancing measures*—Italy shut itself down completely many weeks ago—daily infections and daily deaths do not simply crest and then fall, they hit a peak and then that peak becomes a *weeks-long plateau*.
10/ In Italy, the "plateau" the nation hit—even with draconian social distancing measures far more stringent than what the U.S. (broadly speaking) has done—was around 3,500 to 4,000 new infections daily and 500 to 600 deaths daily. The plateau we're at in America is *much* worse.
11/ In America, after a third spike in new daily infections we hit our *infections* plateau on March 31—just 18 days ago. That plateau is a *horrifying* one: 25,000 to 30,000 new infections daily. Keep in mind that Italy's infections and death-toll plateau has lasted for 4 weeks.
12/ In America, we hit our second *death-toll* plateau 17 to 20 days after our second infection spike: it was 1,200 to 1,400 deaths daily. We are now on our third *death-toll* plateau and it is almost beyond comprehension: 2,000+ deaths daily. We've been around there 11 days now.
13/ The problem with getting that number down is—as noted—death toll is a lagging indicator. If infections sit on a plateau for a long time, the death toll registers it 17-20 days later and then is likely to sit on its own plateau for as long as new infections stayed at *theirs*.
14/ New daily infections hit their third—hopefully *final*—U.S. plateau on March 31: 25,000 to 30,000 new infections daily. If we're like Italy—which used *more draconian measures* than we have—we'll be at this insane new-infection plateau the whole month of April. (God forbid.)
15/ *If* things continue as they have been—if we don't *tighten* our current social distancing measures—there's reason to think that the death-toll plateau we're on now could last *almost* as long as the infection plateau. There's reason to hope it'll be slightly shorter, though.
16/ There's a *chance* some percentage of the rise in new infections was due to the U.S. testing mildly sick people unlikely to die it wasn't testing previously. Unfortunately, evidence suggests the U.S. has *slacked* in testing—it's been flat for April—rather than ramping it up.
17/ The current death-toll plateau—2,000+ daily deaths—is on Day 11, so there's a chance we've 15-20 days of this left (you can do the horrifying math on that).
But I'd add that until the *infection* plateau ends—it hasn't—it's not clear why a "lagging" death-toll plateau would.
But I'd add that until the *infection* plateau ends—it hasn't—it's not clear why a "lagging" death-toll plateau would.
18/ There are many reasons the infection plateau hasn't ended yet—and it seems *none* have to do with increased testing. Rather, we have Trump supporters congregating in churches, in public protests and in places they think—wrongly or not—haven't been or won't be hit by COVID-19.
19/ We also have some states whose governors—under Trump's influence—have increased their state's current and future death tolls by not imposing strict social distancing measures. *All* these deaths must be laid at the feet of Trump and GOP officials—they know what they're doing.
20/ But there's a *sixth* thing medical experts have managed to *occasionally* get into public discourse, but far less commonly than any other fact they've (by fits and starts) pushed through:
6⃣ Our current death-toll data are wrong. Wildly wrong. We are *way* underestimating.
6⃣ Our current death-toll data are wrong. Wildly wrong. We are *way* underestimating.
21/ This under-estimating is so severe that a *single locale*—New York City—recently had to add *3,700* new deaths in its *first* adjustment of its death-toll data, an adjustment that *by itself* increased the total U.S. death toll from COVID-19 at the time by an incredible 17%.
22/ This accidental under-estimating—which is not reflected in any expert modeling (and should be) but is also not result of any bad faith whatsoever—is caused by many factors, including:
1⃣ Not testing people postmortem.
2⃣ Not capturing data for those who die at home.
[cont.]
1⃣ Not testing people postmortem.
2⃣ Not capturing data for those who die at home.
[cont.]
23/
3⃣ Not capturing data from those with co-morbidities whose cause of death may be listed as other than COVID-19.
4⃣ In some few instances, the pace of the pandemic in certain locales may have caused certain jurisdictions to have accidental lapses with their record-keeping.
3⃣ Not capturing data from those with co-morbidities whose cause of death may be listed as other than COVID-19.
4⃣ In some few instances, the pace of the pandemic in certain locales may have caused certain jurisdictions to have accidental lapses with their record-keeping.
24/ If *just* NYC, in just *one* data self-correction, had to add 3,700 deaths to its total, it's hard to even imagine how many deaths are *not included in the official count*—*or* in any of the expert modeling—on a nationwide basis. But we do know the number would be quite high.
25/ The upshot of all this is that non-experts are *lying* about the pandemic to minimize it, and experts are *accidentally* confusing people into thinking things aren't currently as bad as they are and won't be as bad as they're going to be. Both issues *affect public policy*.
26/ Separate from all this, Trump has been *very* successful at keeping medical experts out of the "reopening America" conversation altogether. He insanely—and it *is* insanity—treats that issue as one where the only relevant "experts" are people in business who want a reopening.
27/ So here's what the *medical experts* are trying to tell America about COVID-19 that is relevant to the "reopening" issue, *separate* from how much more horrifying the infection- and death toll-data is than anything most people understand just from watching the news:
[cont.]
[cont.]
28/
1⃣ The virus can travel 16 feet in the air when expelled from a mouth.
2⃣ We don't know how long the virus can hang in air—but it can.
3⃣ We don't know exactly how long the virus stays on porous and nonporous surfaces—but it's at least 24 hours on cardboard, 72 on plastic.
1⃣ The virus can travel 16 feet in the air when expelled from a mouth.
2⃣ We don't know how long the virus can hang in air—but it can.
3⃣ We don't know exactly how long the virus stays on porous and nonporous surfaces—but it's at least 24 hours on cardboard, 72 on plastic.
29/ In view of the foregoing, the danger at your workplace—should it reopen—*isn't* a simple matter of whether you can stand "6 feet" away from coworkers at all times. That's an insanity foisted on the country by a president who's a liar and doesn't care if any of us live or die.
30/ In fact, the dangers in reopened workplaces—dangers attendant to a virus more deadly than the current data inform us, for reasons already noted—are these (and others):
1⃣ Any common surfaces.
2⃣ Any space you can't be *16* feet from all coworkers.
3⃣ Asymptomatic coworkers.
1⃣ Any common surfaces.
2⃣ Any space you can't be *16* feet from all coworkers.
3⃣ Asymptomatic coworkers.
31/ That's right: not only are 25 to 50% of all COVID-19 patients *without symptoms*—meaning they'll show up to work as normal and infect others—and not only do we *not* know how long people shed the virus, we're not even sure if you can *get it twice*.
*And* there's no vaccine.
*And* there's no vaccine.
32/ But there's more—as there's another thing medical experts have only intermittently told Americans (because it's not something anyone's proud of, though experts certainly admit it if asked). It's this: *we've no idea how lethal COVID-19 is*. We *don't know its mortality rate*.
33/ I won't get into CFR—case fatality rate—here. I've done many threads on it—it's complicated. But let's put it this way: *even if you think* we should "take the risk" and reopen workplaces that'll quickly get everyone sick, we *can't* because we *don't know how many will die*.
34/ So what's happening is *far* worse than we think; the problems with reopening workplaces—just based on the matter of virus transmission—are *far* greater than we realize; and if we do what Trump is demanding we've *no idea* how many people will die.
*And* there's no vaccine.
*And* there's no vaccine.
35/ *And* it's a seasonal virus that'll come back *second and subsequent times* until a vaccine, which is—at full deployment—18 months off if we're *very lucky*.
*And* we're not testing enough.
*And* we're not doing contact tracing.
*And* people are breaking social distancing.
*And* we're not testing enough.
*And* we're not doing contact tracing.
*And* people are breaking social distancing.
36/ What I'm saying is that this isn't just really really bad—you all know that. It's that it's *worse* than you think and the media, medical experts, and politicians are (in their very different ways and with their very different intents, some good and some not) misinforming us.
37/ It's in *this* context Fauci announced days ago this is a *seasonal affliction*. It's in *this* context IHME just said some states can't even *start* reopening until *July*. It's in *this* context Trump is sending his cultists out into public, *knowing* they'll infect people.
38/ So let's talk solutions, then.
1⃣ Media must stop reporting *any* content from non-experts that purports to spread expert content but isn't. Folks can pass on what experts are saying, but they can't be reported on if they start sentences—as Trump does—with "I just think..."
1⃣ Media must stop reporting *any* content from non-experts that purports to spread expert content but isn't. Folks can pass on what experts are saying, but they can't be reported on if they start sentences—as Trump does—with "I just think..."
39/
2⃣ We already have some great interlocutors out there for medical experts (@drsanjaygupta is doing a great job—and is of course a doctor himself). But too often, media puts researchers on TV who've never been on TV and don't have communication skills and that helps *no one*.
2⃣ We already have some great interlocutors out there for medical experts (@drsanjaygupta is doing a great job—and is of course a doctor himself). But too often, media puts researchers on TV who've never been on TV and don't have communication skills and that helps *no one*.
40/
3⃣ The "reopening of America" conversation is a *public health conversation*. *Behind the scenes*, businesses and their leaders can work on the logistics of executing the public health schema medical experts deed to them, but they *cannot be involved in timeline production*.
3⃣ The "reopening of America" conversation is a *public health conversation*. *Behind the scenes*, businesses and their leaders can work on the logistics of executing the public health schema medical experts deed to them, but they *cannot be involved in timeline production*.
41/
4⃣ If media keeps off-air non-experts dispensing expert-like proclamations (not simply passing on what experts say)—and if media and experts use good-faith high-functioning-communicator expert-interlocutors—it'll *force* politicians to do what must be done. Which is [cont.]:
4⃣ If media keeps off-air non-experts dispensing expert-like proclamations (not simply passing on what experts say)—and if media and experts use good-faith high-functioning-communicator expert-interlocutors—it'll *force* politicians to do what must be done. Which is [cont.]:
42/
5⃣ However big you thought prior stimulus bills were, they *dwarf* what's actually required—because Congress is going to have to put America on its back and save struggling American families during the *months* more we need to all be at home. Some Democrats already see this.
5⃣ However big you thought prior stimulus bills were, they *dwarf* what's actually required—because Congress is going to have to put America on its back and save struggling American families during the *months* more we need to all be at home. Some Democrats already see this.
43/ But I'm also going to propose an item that'll surprise many people—as it's just about having a *transparent public discourse* with people who are *deadly wrong*.
6⃣ People like Dr. Phil, Dr. Oz, and Trump should *openly* say they are okay with 1 to 2 million Americans dying.
6⃣ People like Dr. Phil, Dr. Oz, and Trump should *openly* say they are okay with 1 to 2 million Americans dying.
44/ I think we would almost do better to *stop* trying to *silence* the maniacs who want to *actively and deliberately* execute public policies that would kill millions of Americans, and *let them say it out loud* and then shame the living sh*t out of them for being *sociopaths*.
45/ Here's what that looks like—for instance—for a journalist: you may have to use metamodern questioning methods, e.g. methods that involve proposing something you *don't believe* to give interviewees a shot to (for once) tell the truth. Someone should do this with Donald Trump.
46/ Ask Trump a question like this (which, as it's predicated on things no one should believe, shouldn't be aired live—nor its answer aired live—but only summarized later on):
"You've said millions may die from a Great Depression. Why not reopen and accept a few million deaths?"
"You've said millions may die from a Great Depression. Why not reopen and accept a few million deaths?"
47/ When you're interviewing someone you *know* believes in something dangerous, you don't shame them *on the front end*, thereby convincing them to lie about what they believe, you ask questions *designed to encourage them* to *say what they actually believe*—no matter how sick.
48/ Understand that a *big* chunk of the GOP thinks that millions of people must die from COVID-19. *Must* die—in order to "save the economy." That view is sociopathic, which is precisely why *we must allow them to say it* rather than permit them to pretend they don't believe it.
49/ By the same token, there's *every* reason to believe a *big* chunk of the expert community sees *total* deaths from COVID-19—assessed retrospectively, a decade on—will be in the *hundreds of thousands*. They *should*—via interlocutors—be given space to spread *that* word too.
50/ This pandemic is a public health crisis.
*And* a humanitarian one. *And* an administrative one. *And* an economic one. *And* a political one. *And* an ethical one. *And* a crisis management one.
*And* a journalistic one. *And* a communications one. We must accept that. /end
*And* a humanitarian one. *And* an administrative one. *And* an economic one. *And* a political one. *And* an ethical one. *And* a crisis management one.
*And* a journalistic one. *And* a communications one. We must accept that. /end
PS/ Just as I finish—BREAKING NEWS consistent with this thread.
1⃣ "Experts still don't know how deadly COVID-19 is."
2⃣ "A new model finds the number of COVID-19 deaths in the U.S. has not yet peaked, and will likely not reach an apex until after May 1." washingtonpost.com/world/2020/04/…
1⃣ "Experts still don't know how deadly COVID-19 is."
2⃣ "A new model finds the number of COVID-19 deaths in the U.S. has not yet peaked, and will likely not reach an apex until after May 1." washingtonpost.com/world/2020/04/…
UPDATE/ Consistent with this thread, the U.S. has just set another new high for daily COVID-19 deaths. The original IHME model—much reported upon—predicted we would hit a peak in deaths about 9 days ago because it didn't consider what *other* experts were saying about "plateaus."