1/ Covid (@UCSF) Chronicles, Day 41
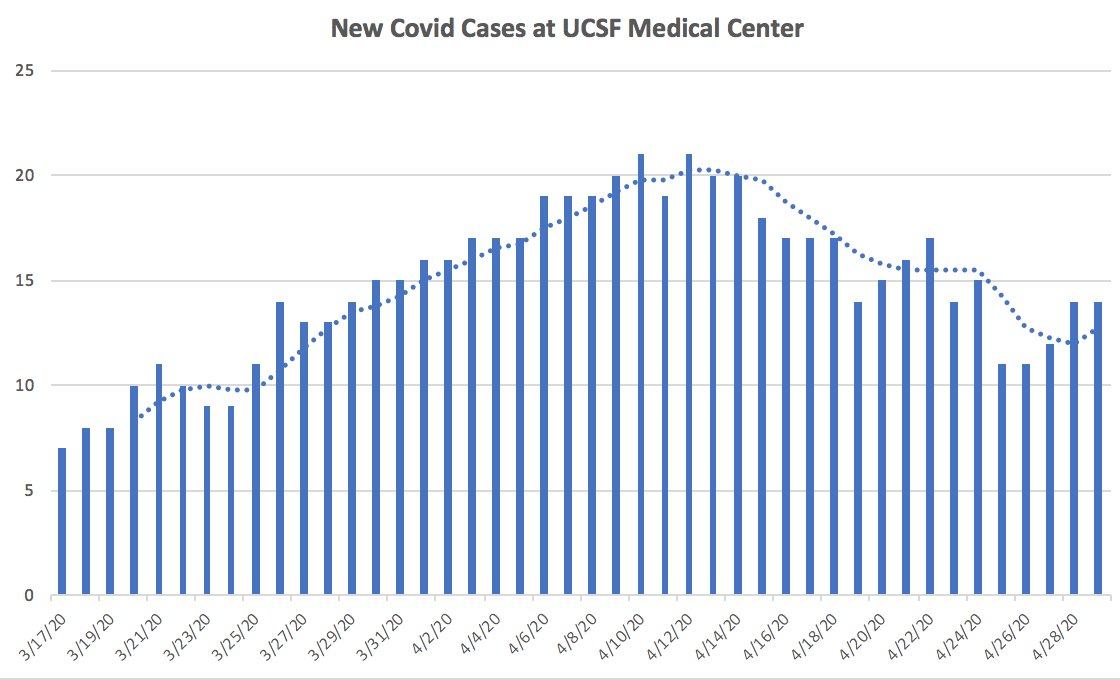
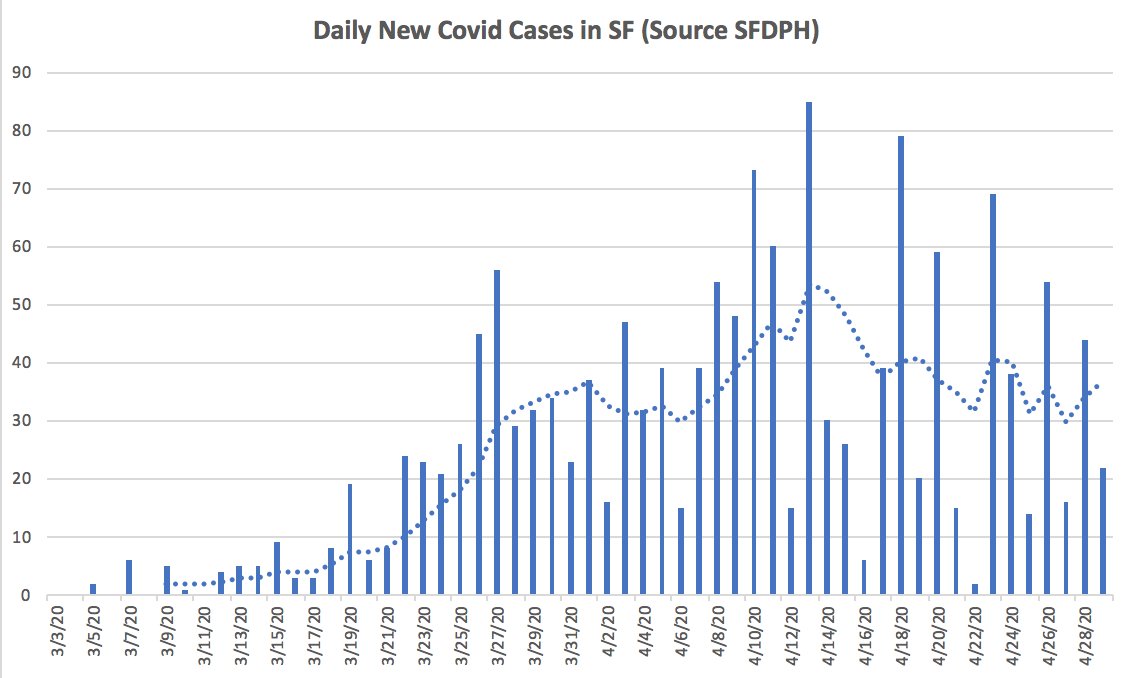
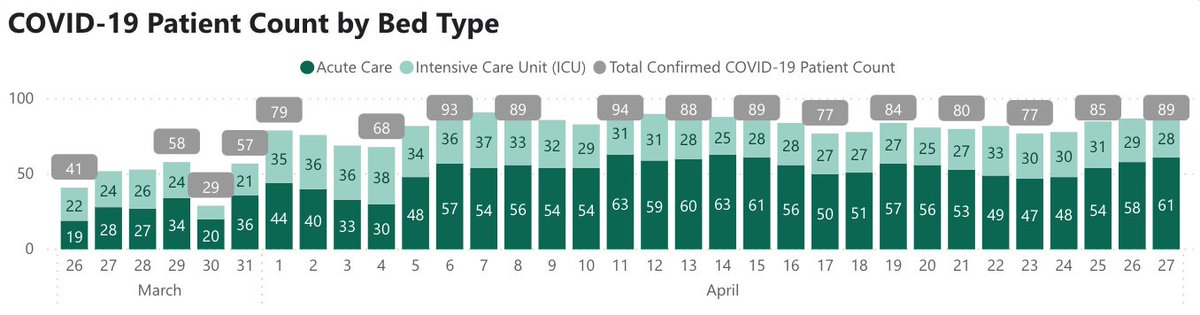
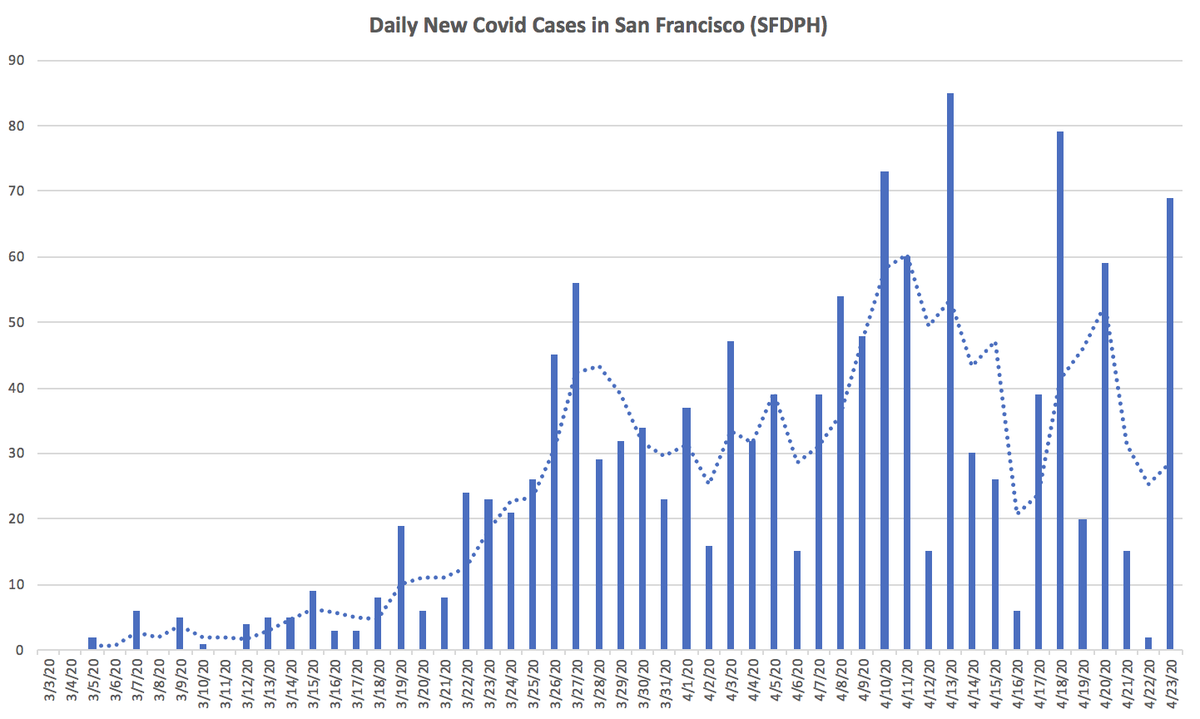
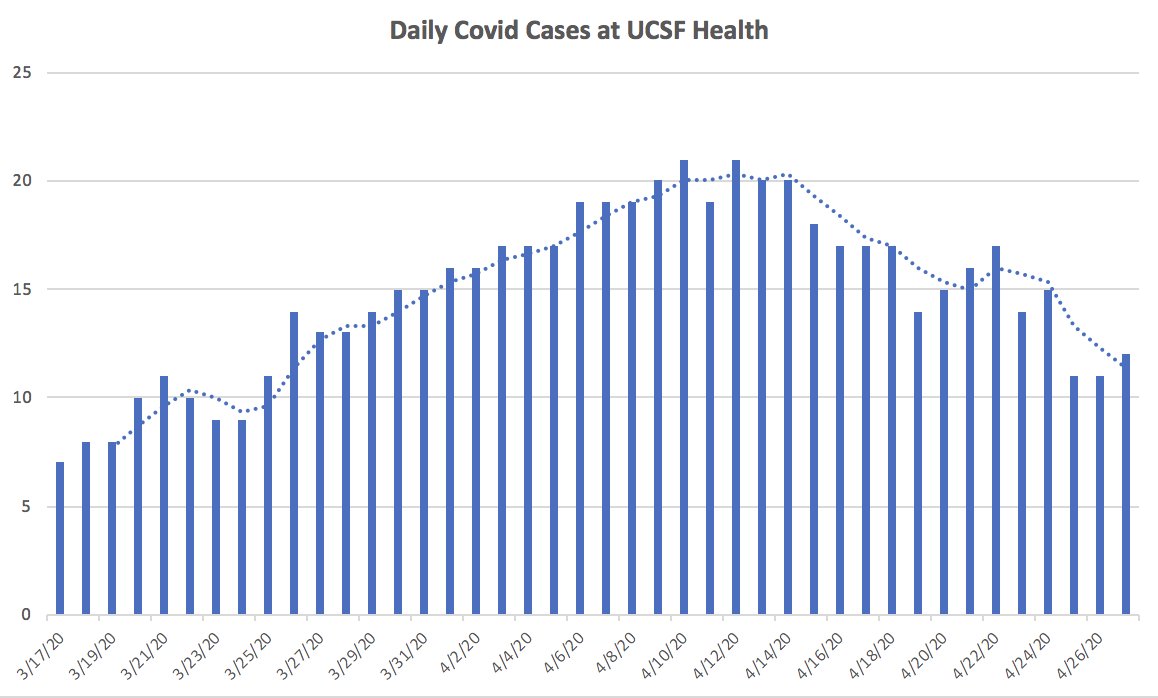
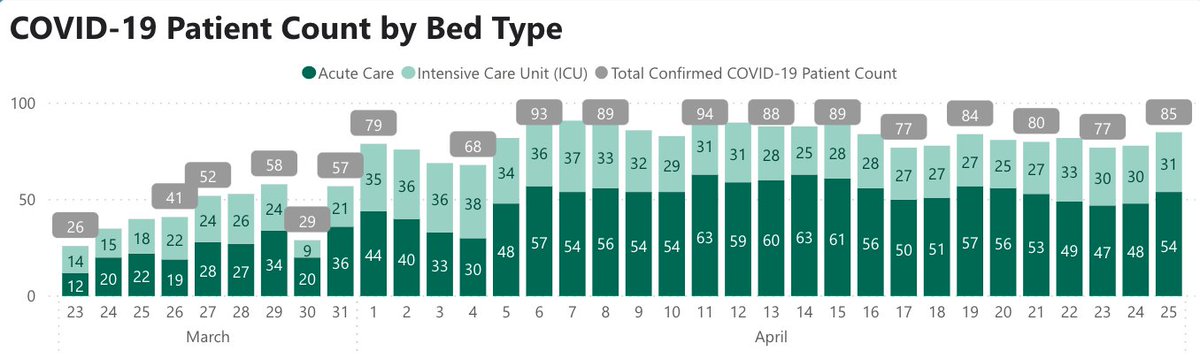
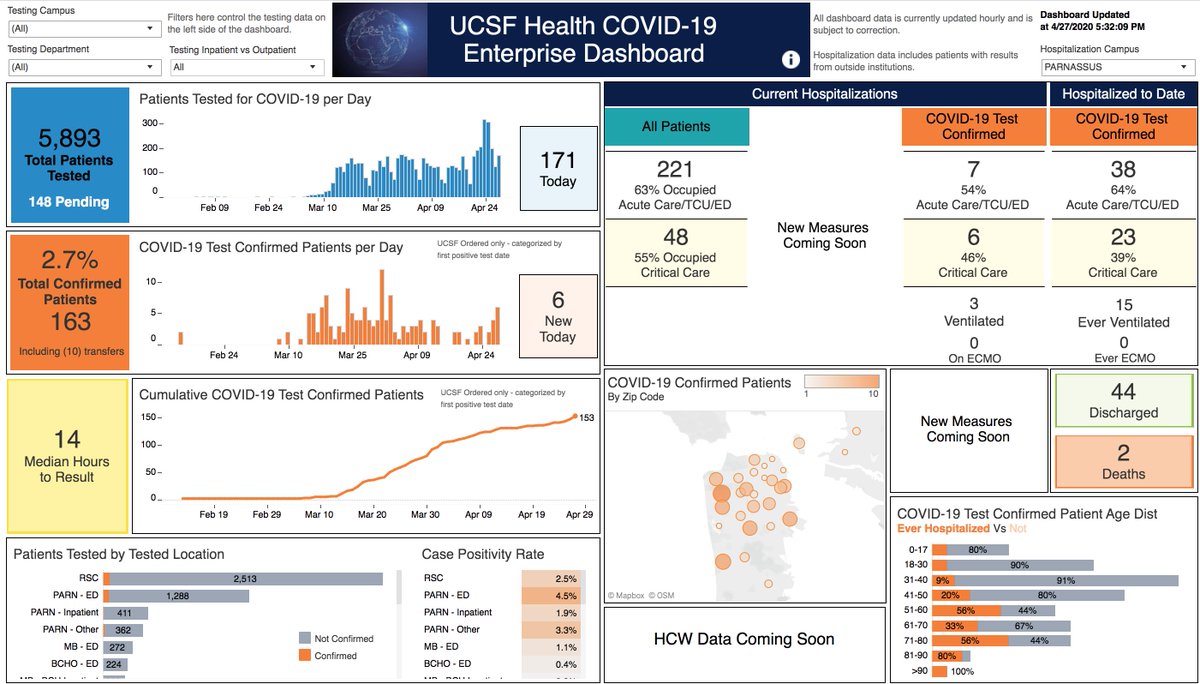
Still stable at @ucsfhospitals. Today, we have 12 patients, 4 on ventilators (Fig on L). Outcomes continue to be good: we’ve discharged 44 patients & had a total of 2 deaths. In SF: 1424 cases (up 16), 23 deaths overall (up 1)(Fig R).
Still stable at @ucsfhospitals. Today, we have 12 patients, 4 on ventilators (Fig on L). Outcomes continue to be good: we’ve discharged 44 patients & had a total of 2 deaths. In SF: 1424 cases (up 16), 23 deaths overall (up 1)(Fig R).
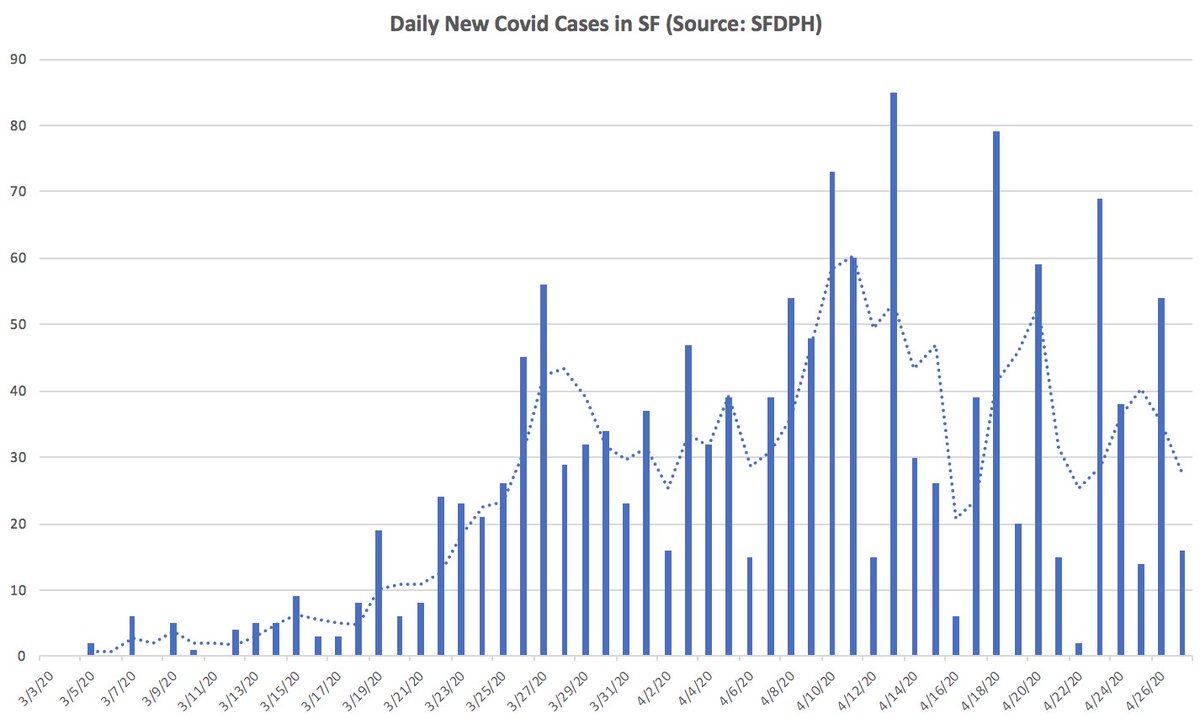
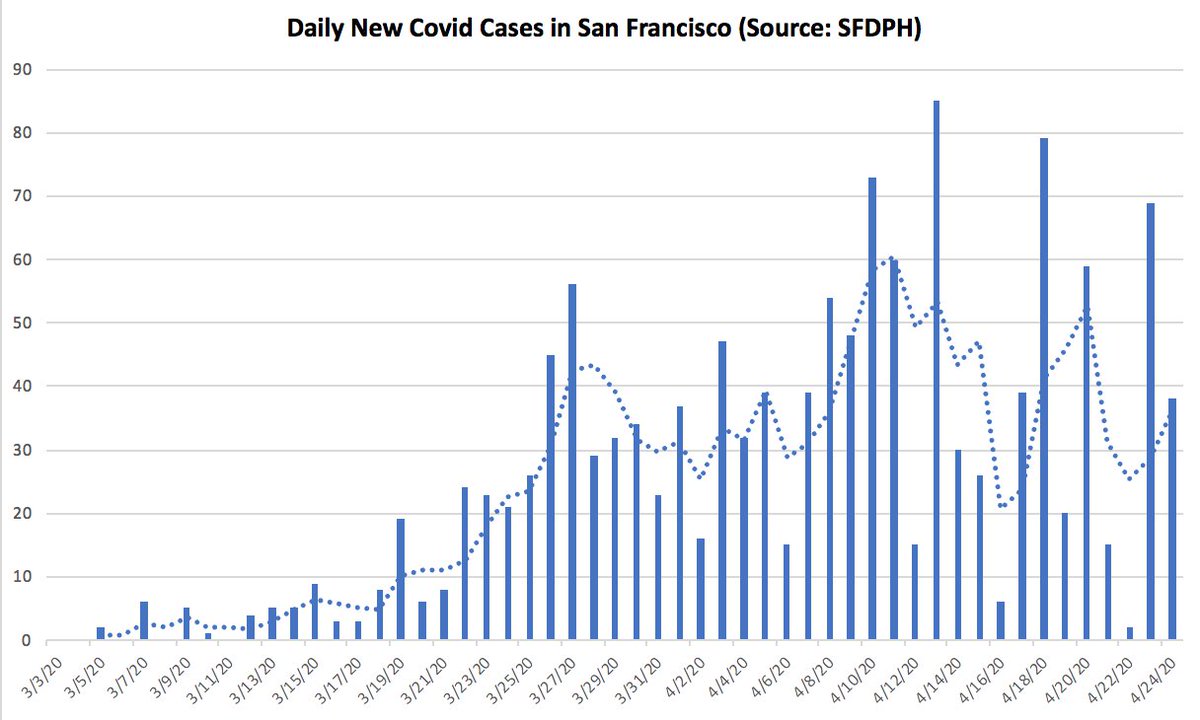
2/ Despite stability @ucsf, SF hospitalizations stubbornly stable (Fig L), as are Bay Area cases (Fig R). Prob why leaders of 6 Bay counties today extended stay-home until 5/31 bit.ly/3cW6Kci Tough call, but our leaders have called ‘em right so far, & earned our trust
3/ I’ll start with a few newsworthy items (#5-8), & then I’ll focus on impact of tech on Covid (& vice versa). Super-long (sorry), but lots to chew on and health tech is my favorite topic…
4/ Much of public health emphasis has been on testing – understandable. But new recs, by @ASlavitt & @ScottGottliebMD n.pr/2xafQCK, focus on contact tracing & quarantine capacity – a crucial component. Important proposal. (More on tech-enabled tracing below, #14-15).
5/ More antibody studies (now from Miami hrld.us/2Y8cpHM) add to data re: undiagnosed cases. Most studies seem to be settling on [true cases = 10-15x diagnosed cases], though false positives likely make this a bit of an overestimate. Much hinges on accuracy of tests….
6/ …which makes crucial a new study by @UCSF’s Alex Marson et al on accuracy of serology tests (data: bit.ly/2ScbIcF; preprint: bit.ly/2xUnyBB; @nytimes: nyti.ms/2VYGAP4). Bottomline: some tests are ok, many aren’t, and bad tests lead to bad decisions.
7/ Last one before going to tech: fine piece by @PamBelluck on saga of Jim Bello, 49 year-old healthy man who spent 1 month on a vent at #MGH nyti.ms/2VKDWh7 Captures randomness of Covid, heroics of care team, and need for trial-and-error given all the uncertainties.
8/ Now to tech, starting w/ AI, the coolest but often overhyped part of health-tech. On @60Minutes last night cbsn.ws/3cQnzoQ: how one Canadian AI company (@helloBlueDot) used Big Data (cases, plane routes, etc) to get an early handle on where Covid might spread…
9/ I found the story a bit hyperbolic – sure, AI might have offered more precise & earlier predictions, but the real question is how the information changes decisions. @60Minutes, @GavinNewsom argued that this AI-based intelligence was our secret weapon in California….
10/ Maybe, but I’m guessing AI was only 1 input (others: talk to experts, read the news). Real secret was leaders who were game to make hard, data-based calls. Here’s piece I wrote w/ Zeke Emanuel on why better AI prediction isn’t enough; it’s what you do. bit.ly/2YBF3hq
11/ As in rest of medicine, relatively little Covid-related AI has entered care settings. One of first tries is Epic’s (bestselling electronic health record) rollout of EHR/AI-based predictor of outcomes, which – sorry to say – scares me a bit bit.ly/2W0aPFi @statnews
12/ Why? While saying which Covid pts may crash is nice, I worry about bias. What if swamped hospitals gave more attention to wealthy white pts than poor black ones; then AI model would find African-Americans are at higher risk of death…. ie, AI can codify bias-driven guidance…
13/ This isn't theoretical. Here are 2 papers (one by @ucsf’s @saramurrayMD @russcucina & me bit.ly/2Y5yUxc ; other by @ucberkeley’s @oziadias bit.ly/2Y9tz87) with real-world examples of how AI-bias can lead to unethical decisions. Important to be cautious w/ AI
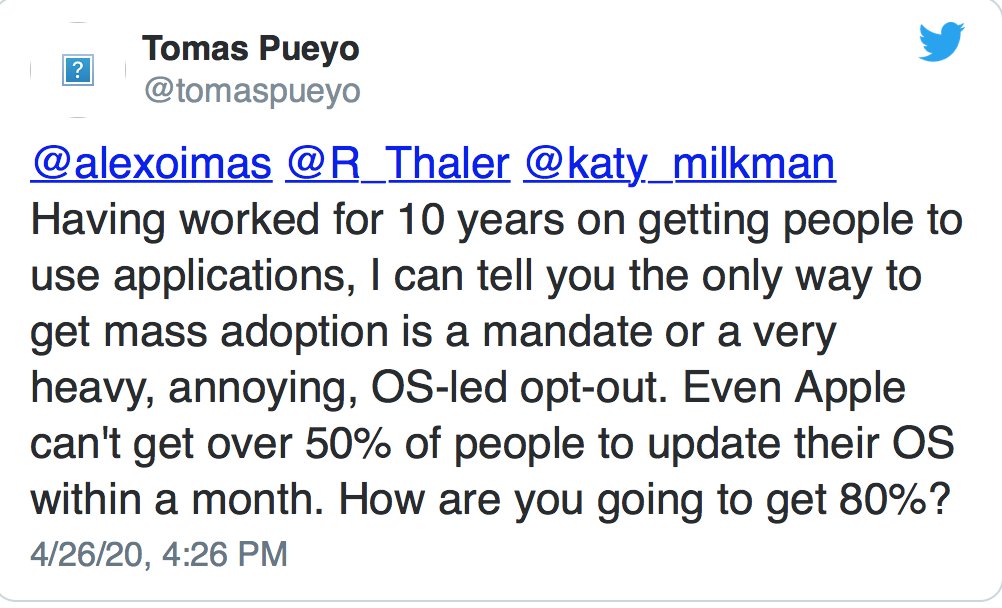
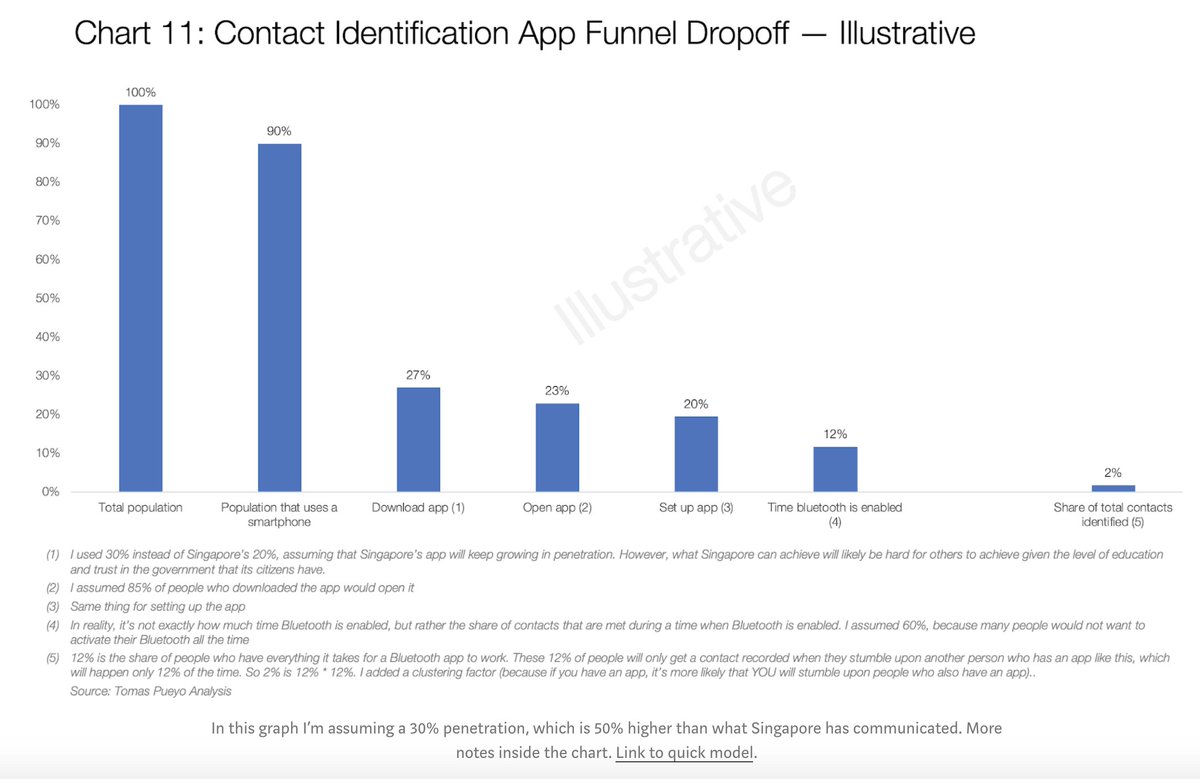
14/ Moving to other tech, I’ve mentioned (#4) contact tracing apps, particularly one being built by @google & @apple bit.ly/2Xr2LQo The tech will probably work fine; big question will be how many people will opt in. To be useful, you need pretty high opt-in rates.
15/ Below, @tomaspueyo shows that even w/ optimistic rates of downloading & opt-in, apps may have small impact on contact tracing bit.ly/34Uhdls I suspect good tracing will still depend mostly on people & shoe-leather, not digital magic, though we might be surprised.
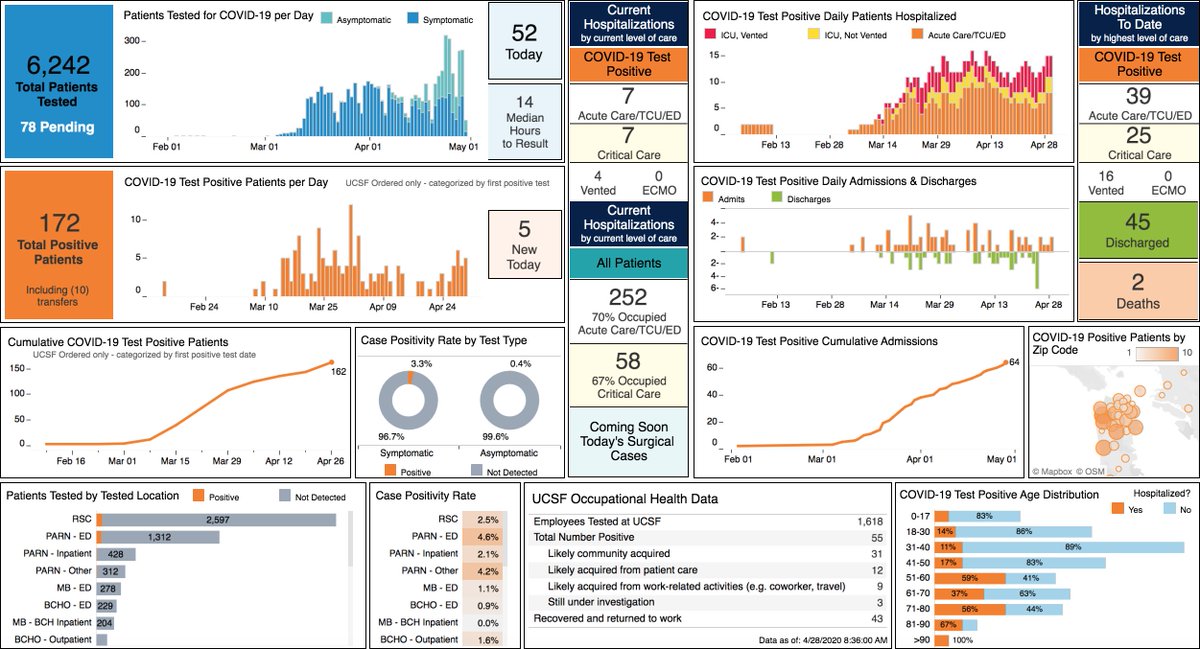
16/ If AI & digital tracing won’t match hype (not because tech doesn’t work, but due to usual problem: darned people & their habits/fears), has any tech been an unambiguous win in Covid era? Sure, 2: data visualization (I know, lots of #dataviz has some AI inside) & telemedicine.
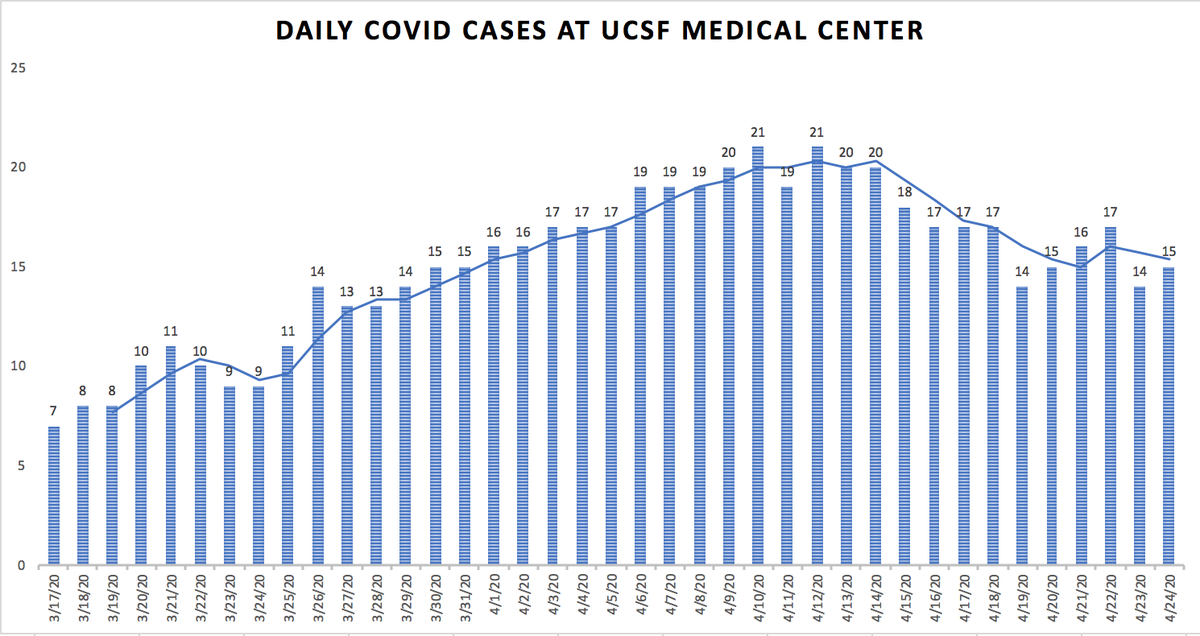
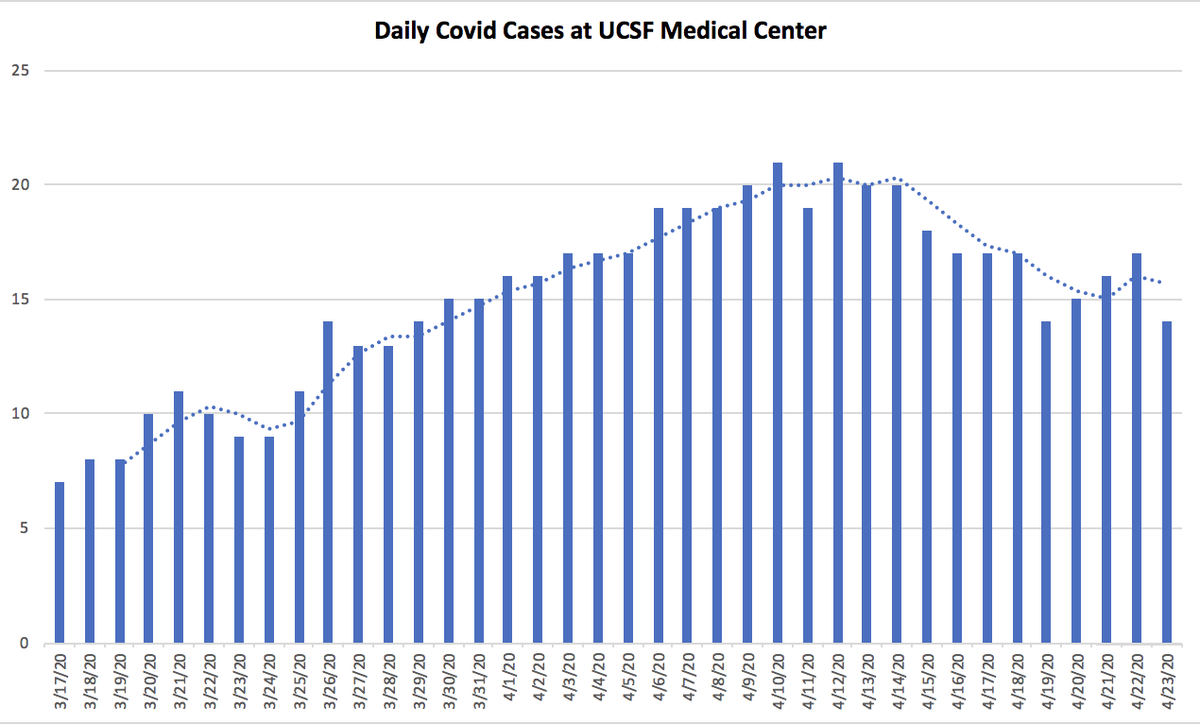
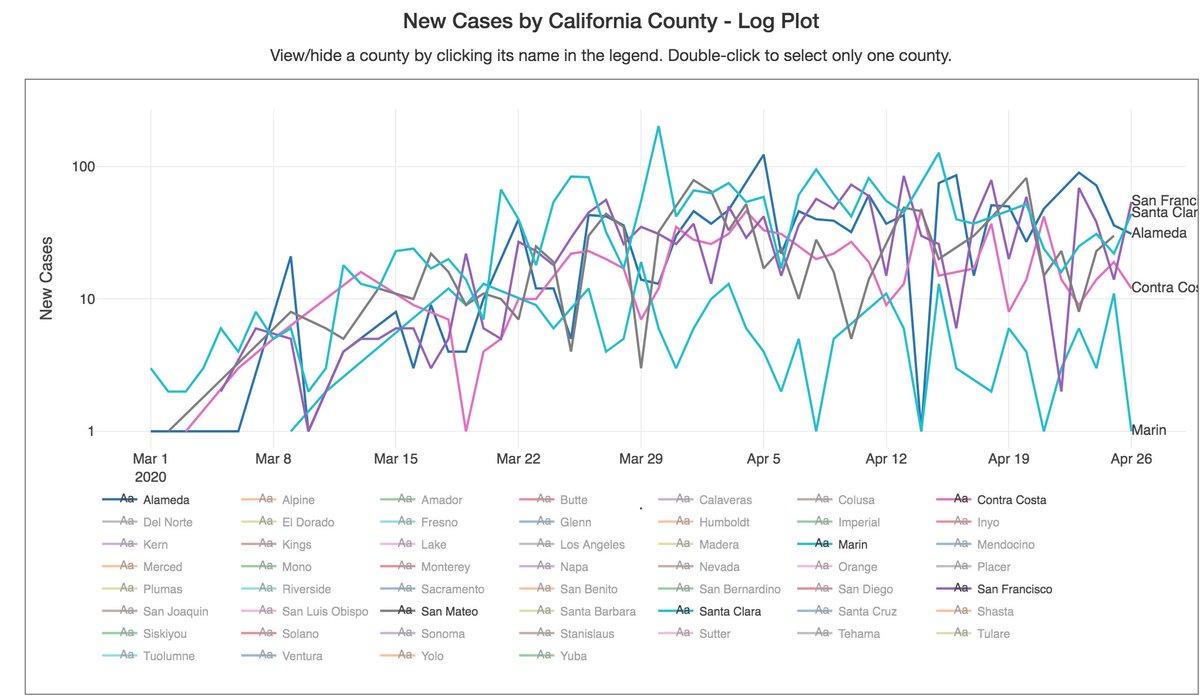
17/ First: #dataviz-meets-healthcare. Here are dashboards I look at daily: 1) our @ucsf data (Fig) by @saramurrayMD; one by @atulbutte et al. w/ data by counties (bit.ly/3eTDzIp). And, of course, the biggies like @JohnsHopkins data, @IHME_UW, & @nytimes
18/ And, of course, the most sobering and dazzling example of Covid #dataviz: public.flourish.studio/visualisation/… By @f_l_o_u_r_i_s_h
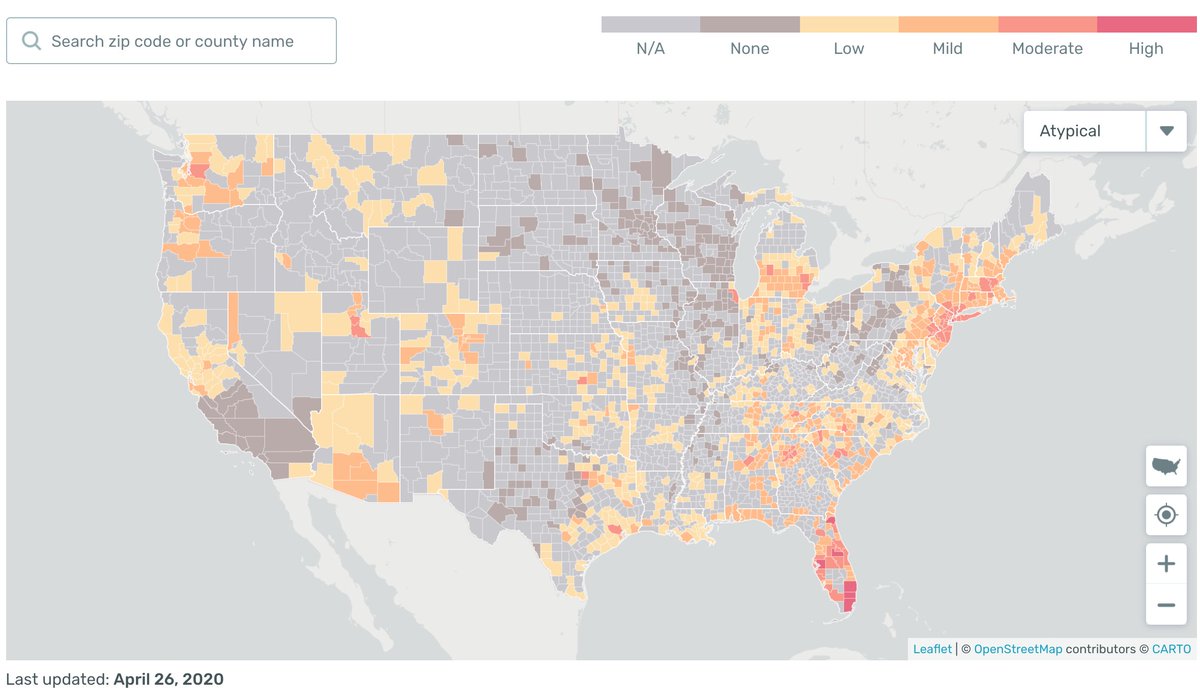
19/ It’s nice seeing digital giants apply talents to Covid. For example, @Kevin & @mikeyk, @instagram founders, built very cool tool rt.live (& bit.ly/2VEBLLM) that tracks virus effective reproduction rate (Rt) in every state. Great stuff for deeper dive.
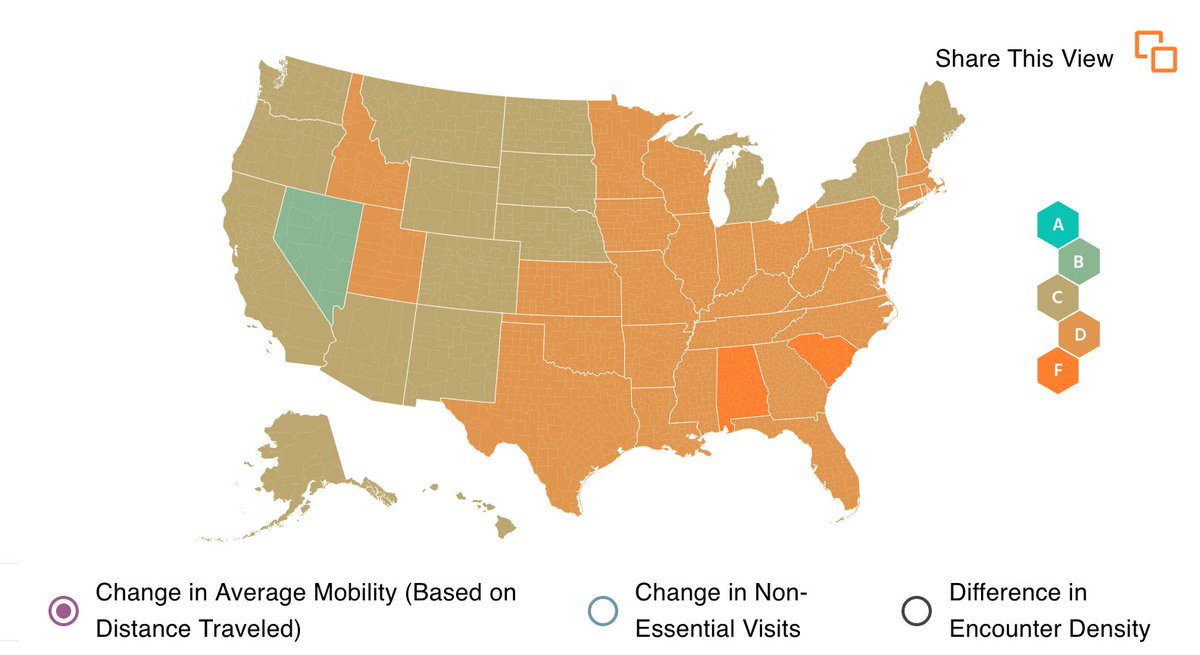
20/ Syndromic surveillance, ie @Kinsa temp map kinsahealth.co, also cool (Fig on L; note, though, only ~50% of Covid pts have fever). And there's behavior surveillance, eg, regional social distancing (Fig R), @unacast. All these need context but can help w/ big picture.
22/ Big question: does telemed simply replace in-person visits (good for pts & saves a few bucks on space/staff... but not transformative). To be transformative, need telemed coupled w/ home monitoring/management, which may prevent exacerbations, ED visits, & hospitalizations.
23/ But for it all to work, we need to monitor home data streams – heart rate/rhythm, weight, blood sugar, BP, O2 saturation, fluid balance, med adherence…Of course we CAN: there are sensors for all this stuff. But, per today’s theme, measurement does not guarantee effectiveness
24/ If these data are sent to a PCP 4x a day (or streamed continuously), every doc I know will quit. Need a new layer of “care traffic controllers” monitoring these data, reacting promptly to outliers (via AI-based algorithms or televisits), & triaging patients to MDs when needed
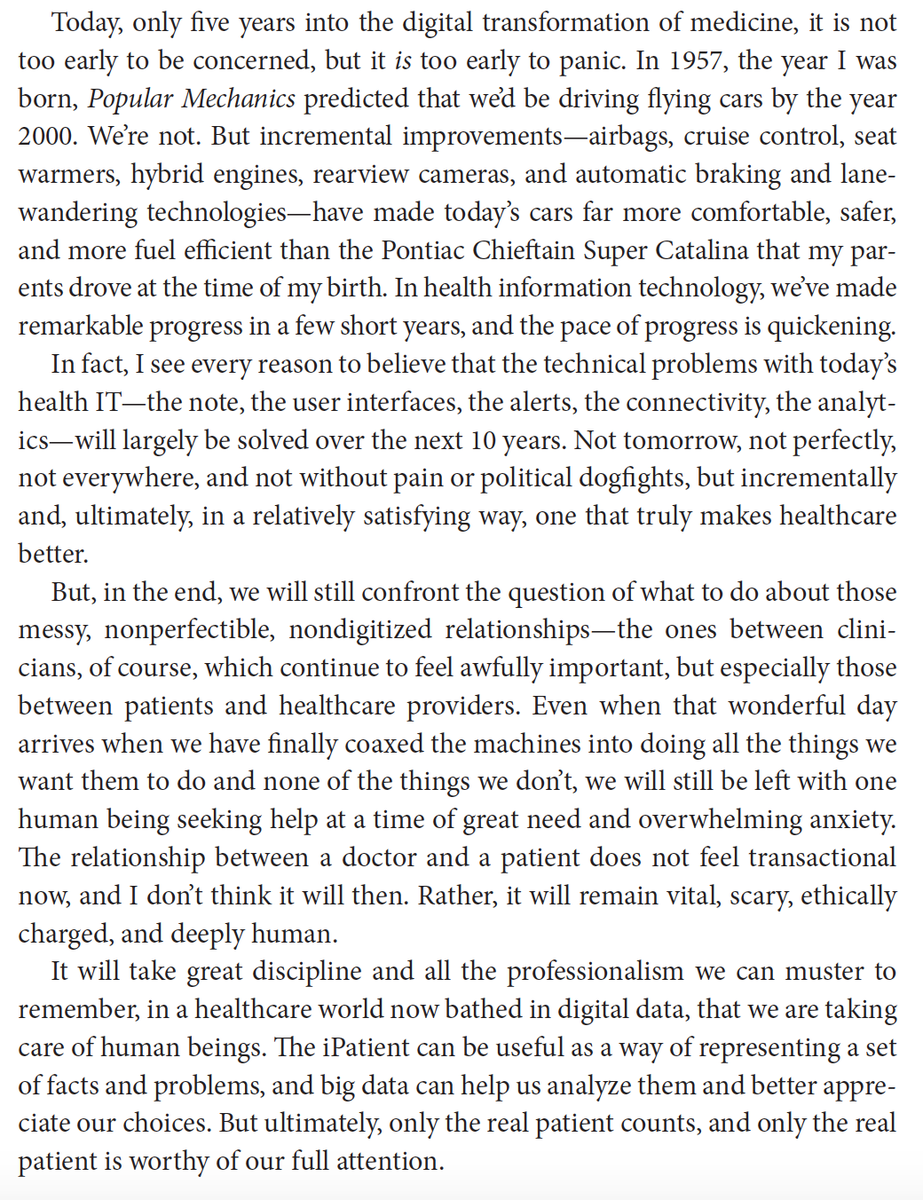
25/ Uber-theme in Tech-Meets-Healthcare: have to get tech right, but that’s the easy part. This clip, from my book “The Digital Doctor” amzn.to/35c32Zq has my thoughts re: the opportunity & challenge. Covid has quickened the pace & raised the stakes.
More Wednesday…
More Wednesday…