"...it is crucial that we establish the pathways involved in the different stages of the inflammatory response to SARS-CoV-2 and determine the contribution of these pathways to ultimate disease outcome."
1/ Possible pathways based on knowns
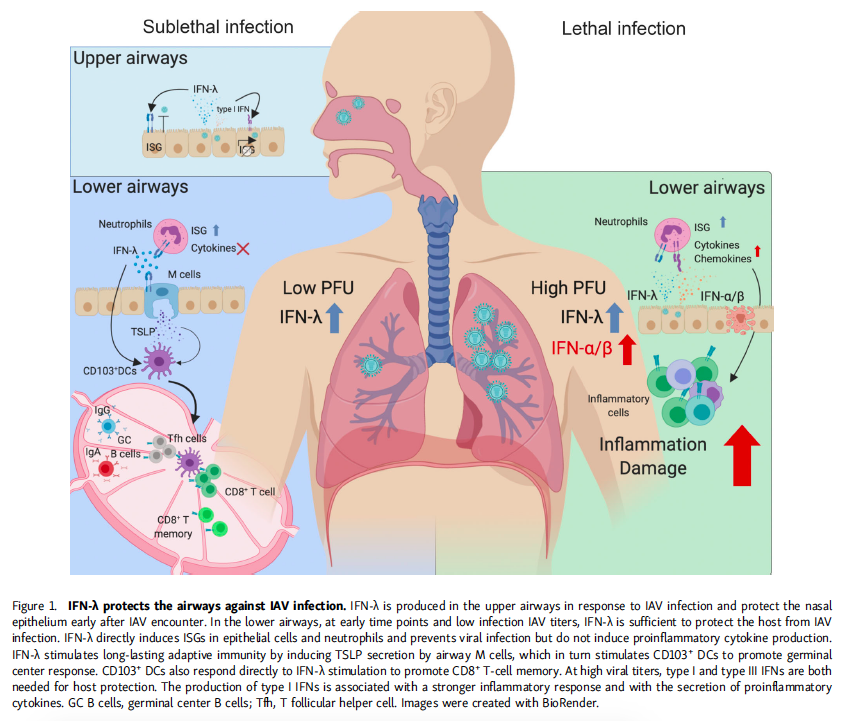
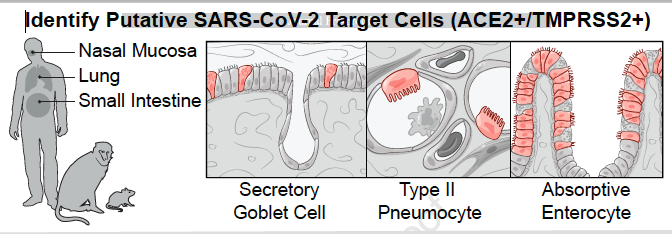
Stage I - Viral entry into upper airway
IFN-λ response restricts viral replication to upper airway
1) Virus cleared early
2) Virus kept in check until seroconversion (~7-10 days)
Asymptomatic or mild outcome.
ncbi.nlm.nih.gov/pubmed/31821443
Stage I - Viral entry into upper airway
IFN-λ response restricts viral replication to upper airway
1) Virus cleared early
2) Virus kept in check until seroconversion (~7-10 days)
Asymptomatic or mild outcome.
ncbi.nlm.nih.gov/pubmed/31821443
2/
Stage 2 - Virus enters lower airway
Could occur 2 ways:
1) Directly, through inhalation
2) If patient has IL-17A mediated inflammation in airway (thread) at time of infection, then IFN-λ⬇️- virus can replicate to higher titer
jimmunol.org/content/201/8/…
Stage 2 - Virus enters lower airway
Could occur 2 ways:
1) Directly, through inhalation
2) If patient has IL-17A mediated inflammation in airway (thread) at time of infection, then IFN-λ⬇️- virus can replicate to higher titer
jimmunol.org/content/201/8/…
3/
If titer low, virus kept in☑️by innate immune response until seroconversion - mild/moderate disease
STAGE 3
If titer high, CoV-2 replicates in type II alveolar pneumocytes, NLRP3 inflammasome triggered
ncbi.nlm.nih.gov/pubmed/?term=2…
sciencedirect.com/science/articl…
If titer low, virus kept in☑️by innate immune response until seroconversion - mild/moderate disease
STAGE 3
If titer high, CoV-2 replicates in type II alveolar pneumocytes, NLRP3 inflammasome triggered
ncbi.nlm.nih.gov/pubmed/?term=2…
sciencedirect.com/science/articl…
4/ Virus inhibits INF response, including INF-λ
Virus replicates relatively unchecked
Virus replicates relatively unchecked
5/
Macrophage recruited to/expanded to lower airway become MH1 activated & inflammatory cytokines produced. Neutrophils recruited.
A major mediator of neutrophil recruitment & lung inflammation is IL-17A.
Macrophage recruited to/expanded to lower airway become MH1 activated & inflammatory cytokines produced. Neutrophils recruited.
A major mediator of neutrophil recruitment & lung inflammation is IL-17A.
6/
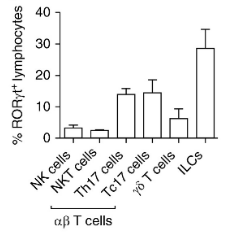
Based on work #inmice the major IL-17A producing cells following NLRP3 activation are RORγt innate lymphoid cells (ILCs).
More about ILCs in thread below
Based on work #inmice the major IL-17A producing cells following NLRP3 activation are RORγt innate lymphoid cells (ILCs).
More about ILCs in thread below
6/
Dysregulation leads to mix of pro and anti-inflammatory cytokines to be produced (cytokine storm). ROS generation & neutrophil degranulation could promote NET formation, possibly contributing to observed thrombosis.
This is all BEFORE seroconversion (~ day 7-10)
Dysregulation leads to mix of pro and anti-inflammatory cytokines to be produced (cytokine storm). ROS generation & neutrophil degranulation could promote NET formation, possibly contributing to observed thrombosis.
This is all BEFORE seroconversion (~ day 7-10)
7/
Linking out 2 thread to end - but punchline:
STAGE 3 needs to be avoided at all costs.
2 ways to achieve:
1)prevent people from inhaling high virus titer
2)nuke inflammation in the respiratory vasculature well BEFORE exposure so IFN-λ is full online
Linking out 2 thread to end - but punchline:
STAGE 3 needs to be avoided at all costs.
2 ways to achieve:
1)prevent people from inhaling high virus titer
2)nuke inflammation in the respiratory vasculature well BEFORE exposure so IFN-λ is full online