
Does dizziness make you feel dizzy?
It's complicated, so here is a #Tweetorial on Dizziness!
#MedEd #MedStudentTwitter #MedStudents #neurology
cc: @Tracey1milligan @MadSattinJ @CPSolvers @rabihmgeha @DxRxEdu @AANMember @ContinuumAAN 1/
It's complicated, so here is a #Tweetorial on Dizziness!
#MedEd #MedStudentTwitter #MedStudents #neurology
cc: @Tracey1milligan @MadSattinJ @CPSolvers @rabihmgeha @DxRxEdu @AANMember @ContinuumAAN 1/
HISTORY
Try to determine if the dizziness falls into one of these categories:
1 Vertigo (sense of movement)= neurologic or inner ear
2 Light-headed=CV related
3 Dysequilibrium=gait issue
4 other=anxiety
This classic paper is worth the read ncbi.nlm.nih.gov/pubmed/4401538
2/
Try to determine if the dizziness falls into one of these categories:
1 Vertigo (sense of movement)= neurologic or inner ear
2 Light-headed=CV related
3 Dysequilibrium=gait issue
4 other=anxiety
This classic paper is worth the read ncbi.nlm.nih.gov/pubmed/4401538
2/
But the history for type of dizziness is not sensitive/specific, as the work of @DNewmanToker has shown jscholarship.library.jhu.edu/bitstream/hand… Note title: “Why “What do you mean by ‘dizzy’?” Should Not Be the First Question You Ask”
Still it's a good place to start...
3/
Still it's a good place to start...
3/
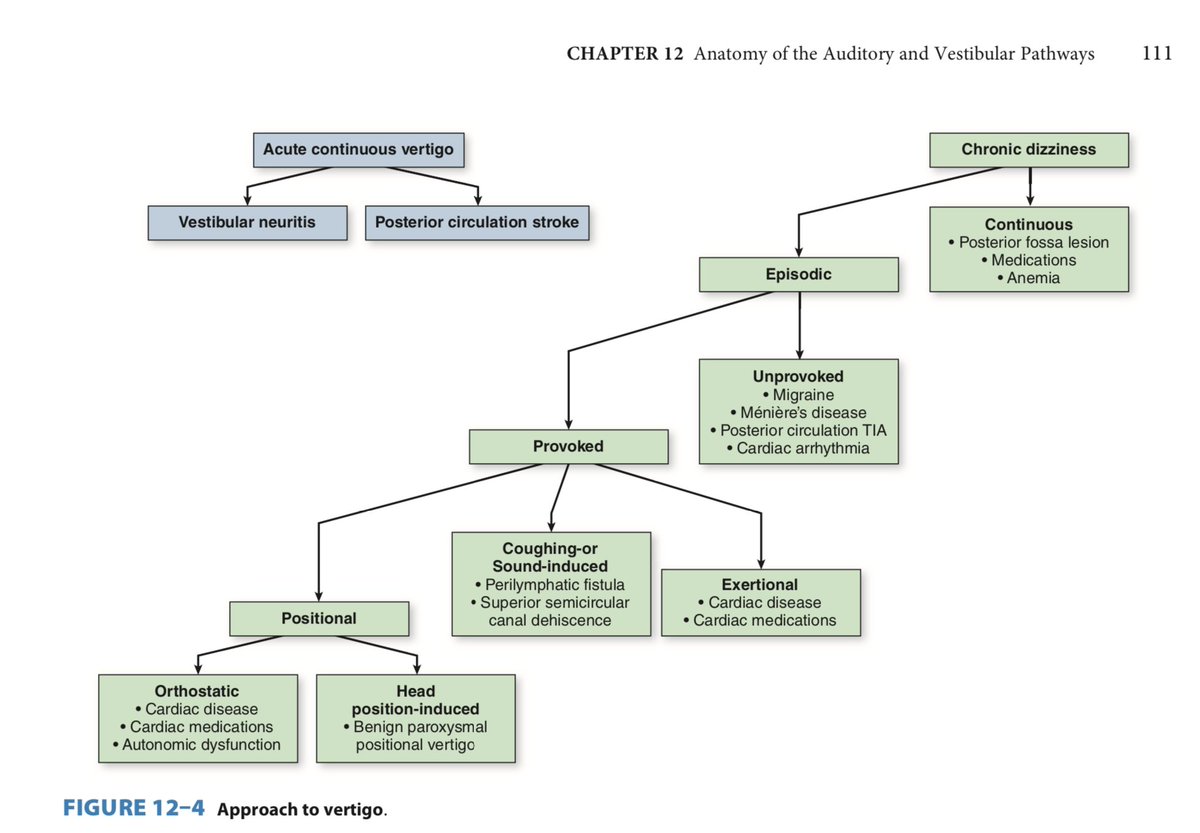
History should also address TIMING and TRIGGERS
For timing: Acute v chronic?
(We’ll come back to acute)
For chronic: continuous v episodic
For episodic: unprovoked v provoked
If provoked: provoked by what? (triggers)
See attached flow chart from amazon.com/Lange-Clinical…
4/
For timing: Acute v chronic?
(We’ll come back to acute)
For chronic: continuous v episodic
For episodic: unprovoked v provoked
If provoked: provoked by what? (triggers)
See attached flow chart from amazon.com/Lange-Clinical…
4/
Acute is a trickier but the stakes are high!
Is it a life-threatening posterior circulation stroke or a benign case of vestibular neuritis?
@DNewmanToker to the rescue with the HINTS exam: ncbi.nlm.nih.gov/pubmed/19762709
5/
Is it a life-threatening posterior circulation stroke or a benign case of vestibular neuritis?
@DNewmanToker to the rescue with the HINTS exam: ncbi.nlm.nih.gov/pubmed/19762709
5/
HINTS is more sensitive and specific than MRI to detect stroke in a patient presenting with acute continuous vertigo. Exam beats technology! Yay neuro exam!
HINTS stands for
Head Impulse
Nystagmus
Test of Skew
6/
HINTS stands for
Head Impulse
Nystagmus
Test of Skew
6/
To understand these we need to understand a little vestibular neuroanatomy
When you turn your head to the left, your eyes turn to the right
When you turn your head to the right your eyes turn to the leift.
This is the Vestibulo-ocular reflex or VOR.
7/
When you turn your head to the left, your eyes turn to the right
When you turn your head to the right your eyes turn to the leift.
This is the Vestibulo-ocular reflex or VOR.
7/
VOR anatomy/physiology:
Head movement detected in inner ear, transmitted to brainstem by CN 8, CN 8 communicates with CN 3/4/6 to move eyes conjugately in direction opposite head motion.
Brain knows direction head is turning by COMPARING the activity in the L and R CN 8.
8/
Head movement detected in inner ear, transmitted to brainstem by CN 8, CN 8 communicates with CN 3/4/6 to move eyes conjugately in direction opposite head motion.
Brain knows direction head is turning by COMPARING the activity in the L and R CN 8.
8/
If we turn head to the LEFT, L CN8 gets more excited. Brain detects L>R = head turn to left->sends eyes to right
If we turn head to the RIGHT, R CN8 gets more excited. Brain detects R>L = head turn to right->sends eyes to LEFT
Got it?
9/
If we turn head to the RIGHT, R CN8 gets more excited. Brain detects R>L = head turn to right->sends eyes to LEFT
Got it?
9/
Just making sure you've got it....? It will help understand the HI and N of HINTS
Also note:
Both CN8s are tonically active at baseline --you'll see why that's important...
10/
Also note:
Both CN8s are tonically active at baseline --you'll see why that's important...
10/
Now imagine a case of vestibular neuritis, usually unilateral.
Let’s say it’s on the LEFT
So left CN 8 is not working well and its baseline tonic activity therefore stops
BUT healthy RIGHT CN8 continues its tonic activity!
So the brain sees: R> L (i.e., something > 0)…
11/
Let’s say it’s on the LEFT
So left CN 8 is not working well and its baseline tonic activity therefore stops
BUT healthy RIGHT CN8 continues its tonic activity!
So the brain sees: R> L (i.e., something > 0)…
11/
So the brain THINKS the head is turning to the RIGHT and send the eyes to the LEFT…
but the head ISN'T turning so we flick the eyes back to the RIGHT…
deviate to left, flick to right…deviate to left flick to right.
It’s nystagmus!
12/
but the head ISN'T turning so we flick the eyes back to the RIGHT…
deviate to left, flick to right…deviate to left flick to right.
It’s nystagmus!
12/
With a unilateral vestibular lesion, the nystagmus maintains CONSTANT direction of fast phase:
Slow phase toward abnormal side and fast phase toward normal side (just like normal cold calorics).
So nystagmus has a CONSTANT direction in a unilateral peripheral etiology.
13/
Slow phase toward abnormal side and fast phase toward normal side (just like normal cold calorics).
So nystagmus has a CONSTANT direction in a unilateral peripheral etiology.
13/
CENTRAL nystagmus comes in various forms. But for acute vertigo: just know that central causes of vertigo lead to DIRECTION-CHANGING nystagmus:
the fast phase is ALWAYS in the direction of gaze: left beating on left gaze; right beating on right gaze…
14/
the fast phase is ALWAYS in the direction of gaze: left beating on left gaze; right beating on right gaze…
14/
So this is the N of HINTS:
Direction-changing nystagmus in acute onset vertigo = concerning for stroke.
Nystagmus with fast phase in same direction in all positions of gaze = peripheral
15/
Direction-changing nystagmus in acute onset vertigo = concerning for stroke.
Nystagmus with fast phase in same direction in all positions of gaze = peripheral
15/
Now for the head impulse test (HIT):
Asking patient to fixate on your nose, move their head briskly to each side: eyes should instantly move in direction opposite to head movement to stay on nose.
16/
Asking patient to fixate on your nose, move their head briskly to each side: eyes should instantly move in direction opposite to head movement to stay on nose.
16/
Let’s come back to a case of unilateral LEFT sided vestibular neuritis.
When we move the head to the left, the CN8 isn’t working to transmit the message to the eyes that the head has moved…
so the eyes move with the head and have to catch up to find the nose= abnormal...
17/
When we move the head to the left, the CN8 isn’t working to transmit the message to the eyes that the head has moved…
so the eyes move with the head and have to catch up to find the nose= abnormal...
17/
So an abnormal HIT is actually a REASSURING sign of peripheral etiology of vertigo.
It’s a NORMAL HIT that’s worrisome in the case of acute vertigo!
*Note NORMAL HIT in acute vertigo = worry about stroke!*
18/
It’s a NORMAL HIT that’s worrisome in the case of acute vertigo!
*Note NORMAL HIT in acute vertigo = worry about stroke!*
18/
Skew is complicated. Let’s just say if it’s present think CENTRAL. But what is it?
If the eyes are looking in wildly different directions it’s not hard to call it central.
19/
If the eyes are looking in wildly different directions it’s not hard to call it central.
19/
But you can find subtle skew by doing a cover-uncover test, moving the hand back and forth between the eyes and seeing if they subtly deviate up for down when uncovered.
If so, test is positive...in acute vertigo, positive test = concerning for stroke!
20/
If so, test is positive...in acute vertigo, positive test = concerning for stroke!
20/
How to remember the HINTS signs?! @DNewmanToker reminds us HINTS are to detect I.N.F.A.R.C.T., standing for
Impulse Normal
Fast-phase-of-nystagmus Alternating
Refixation on Cover Test…
21/
Impulse Normal
Fast-phase-of-nystagmus Alternating
Refixation on Cover Test…
21/
So a normal HIT, direction changing nystagmus, or skew in a patient with acute vertigo is highly concerning for posterior circulation infarct…even if the MRI is negative in the first 24 hours.
(note this applies only to acute continuous vertigo)
Feeling dizzy?
22/
(note this applies only to acute continuous vertigo)
Feeling dizzy?
22/

