
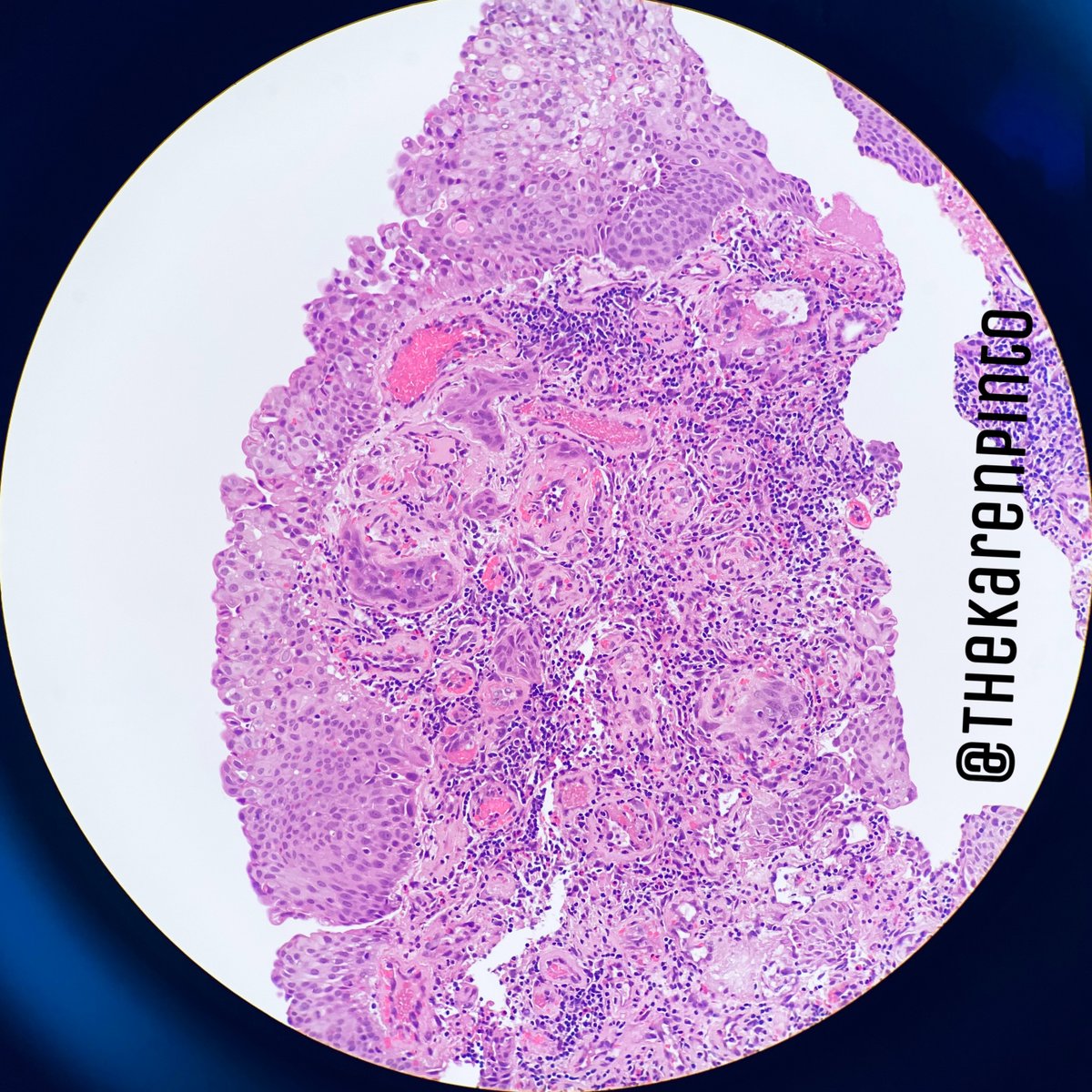
History: Female, 50-ish, presented with hematuria.
Cystoscopy: Congested mucosa with bleeding ulcers
Biopsy from urinary bladder lesion
#pathology #GUPath
Cystoscopy: Congested mucosa with bleeding ulcers
Biopsy from urinary bladder lesion
#pathology #GUPath
What should I do?
I should call the surgeon
“Did the patient have urinary bladder cancer before?”
NO
Patient had cervix cancer, a year back
“Did the patient have urinary bladder cancer before?”
NO
Patient had cervix cancer, a year back




What should I consider now?
1. This could be a new urinary bladder primary
2. This could be metastasis from cervix
3. This is benign
1. This could be a new urinary bladder primary
2. This could be metastasis from cervix
3. This is benign
You should then ask the surgeon, if she received radiation for her cervix cancer
YES
So this is benign
YES
So this is benign
This is a classic case of RADIATION CYSTITIS which occurred due to her prior therapy
Radiation can be given for cancers of urinary bladder, uterus, ovaries, cervix, prostate, colon, rectum etc.
Radiation for any pelvic tumor, will show changes in the colon & urinary bladder.
Radiation can be given for cancers of urinary bladder, uterus, ovaries, cervix, prostate, colon, rectum etc.
Radiation for any pelvic tumor, will show changes in the colon & urinary bladder.
How does it present?
1. Increased frequency
2. Urgency
3. Voiding pain
4. Hematuria
1. Increased frequency
2. Urgency
3. Voiding pain
4. Hematuria
Within what period of receiving radiation, should I attribute these changes to it?
Acute: 3-6 weeks
Chronic: 6 months to 20 YEARS
Acute: 3-6 weeks
Chronic: 6 months to 20 YEARS
What are the clues which I should have seen to make this diagnosis?
Radiation causes changes in all the layers so let’s go one by one
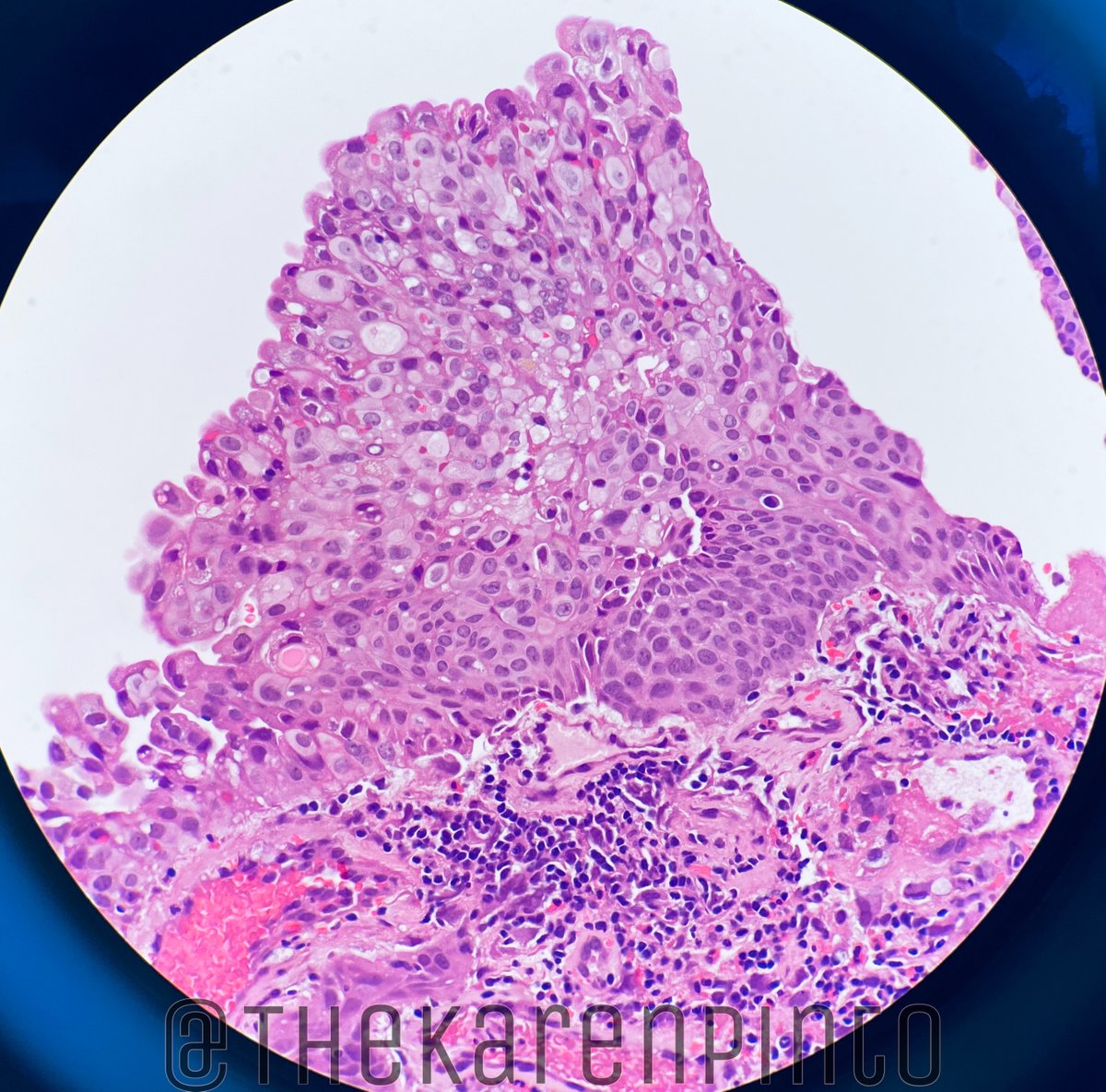
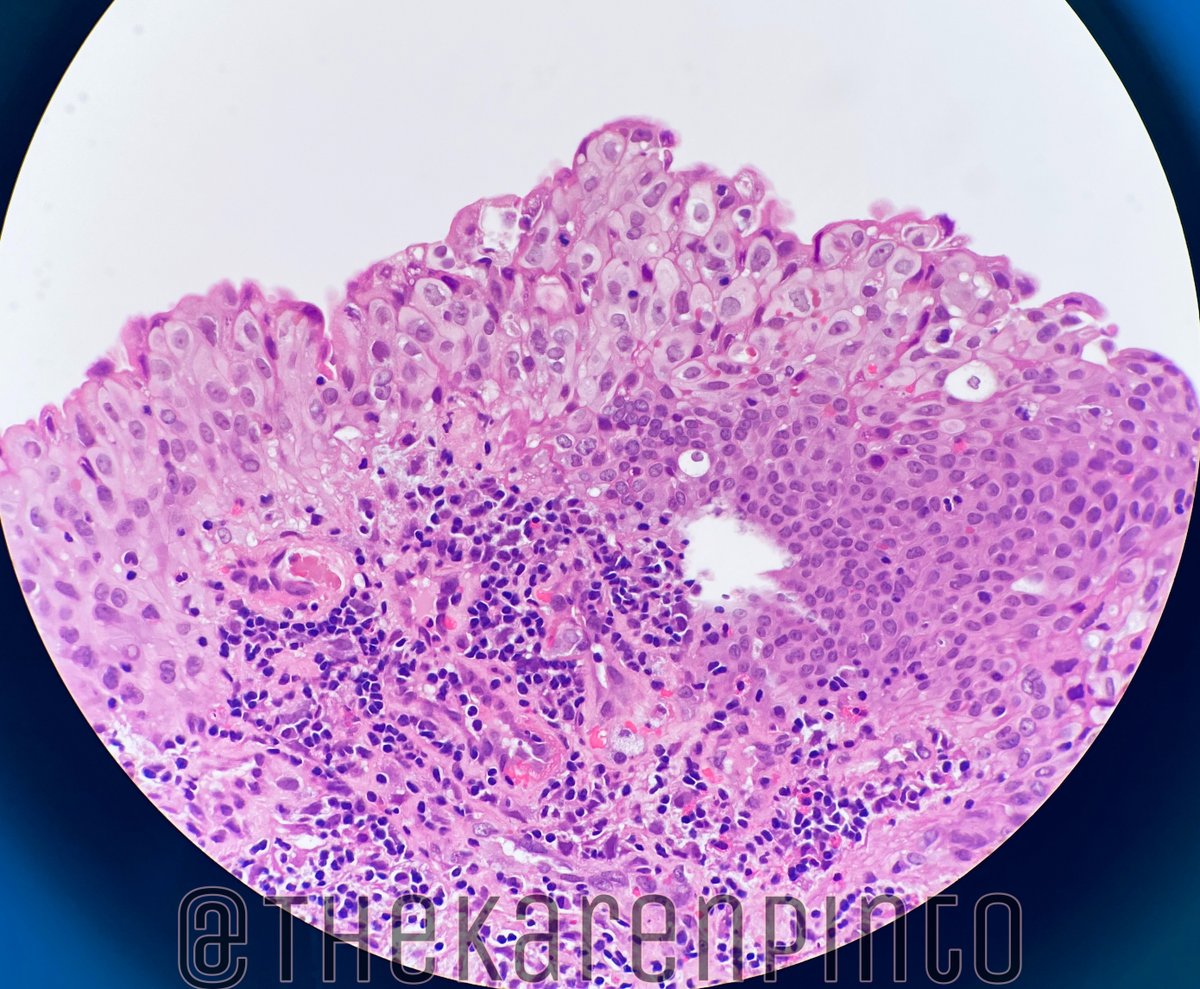
EPITHELIUM:
1. Reactive changes = mitosis
2. Degenerative changes:
- vacuoles (nuclear + cyto)
- smudgy chromatin
- karyorrhexis
Radiation causes changes in all the layers so let’s go one by one
EPITHELIUM:
1. Reactive changes = mitosis
2. Degenerative changes:
- vacuoles (nuclear + cyto)
- smudgy chromatin
- karyorrhexis




3. You can also see the loss of polarization, bizarre nuclei, mitoses = it’s NOT carcinoma in situ


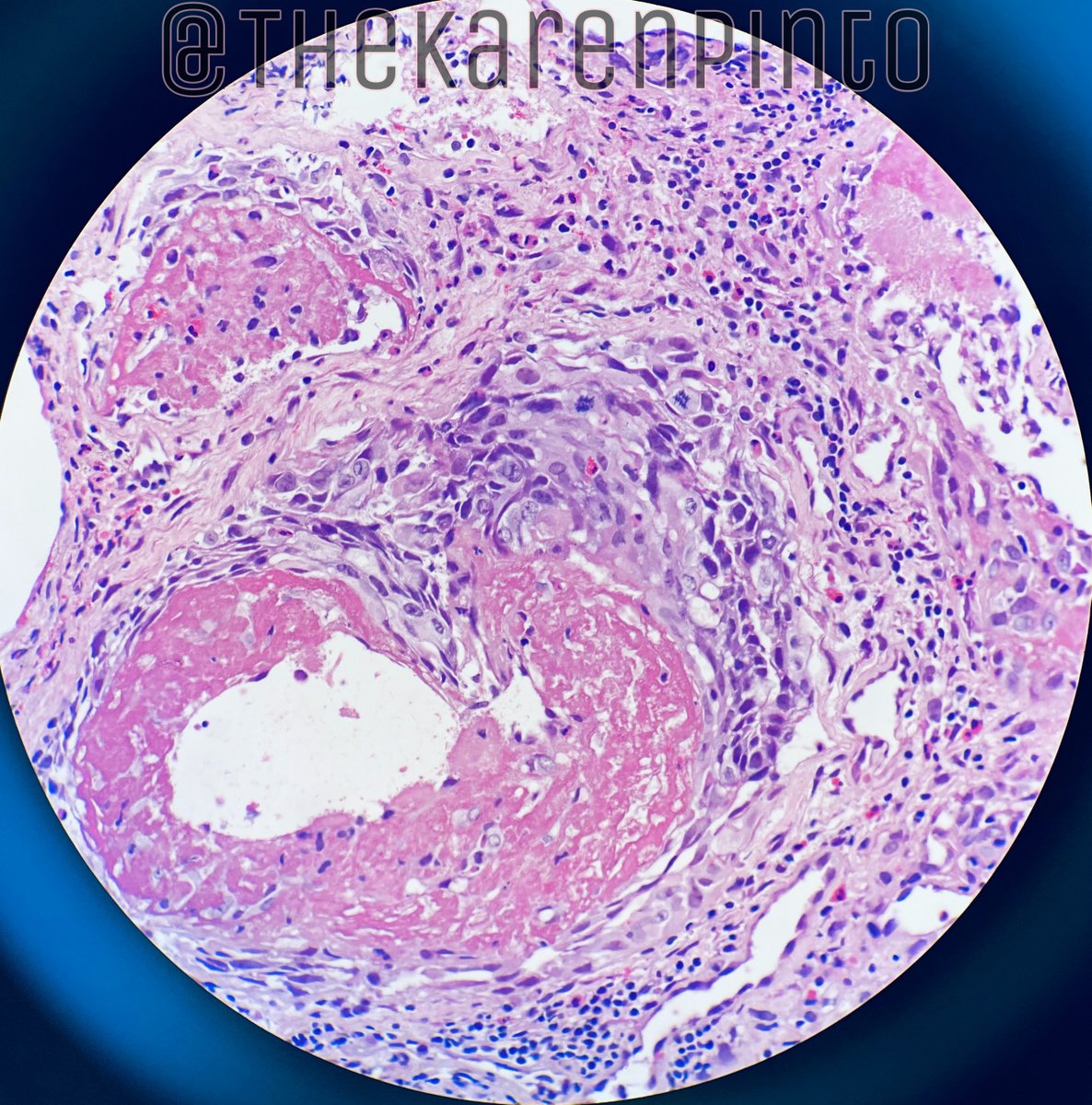
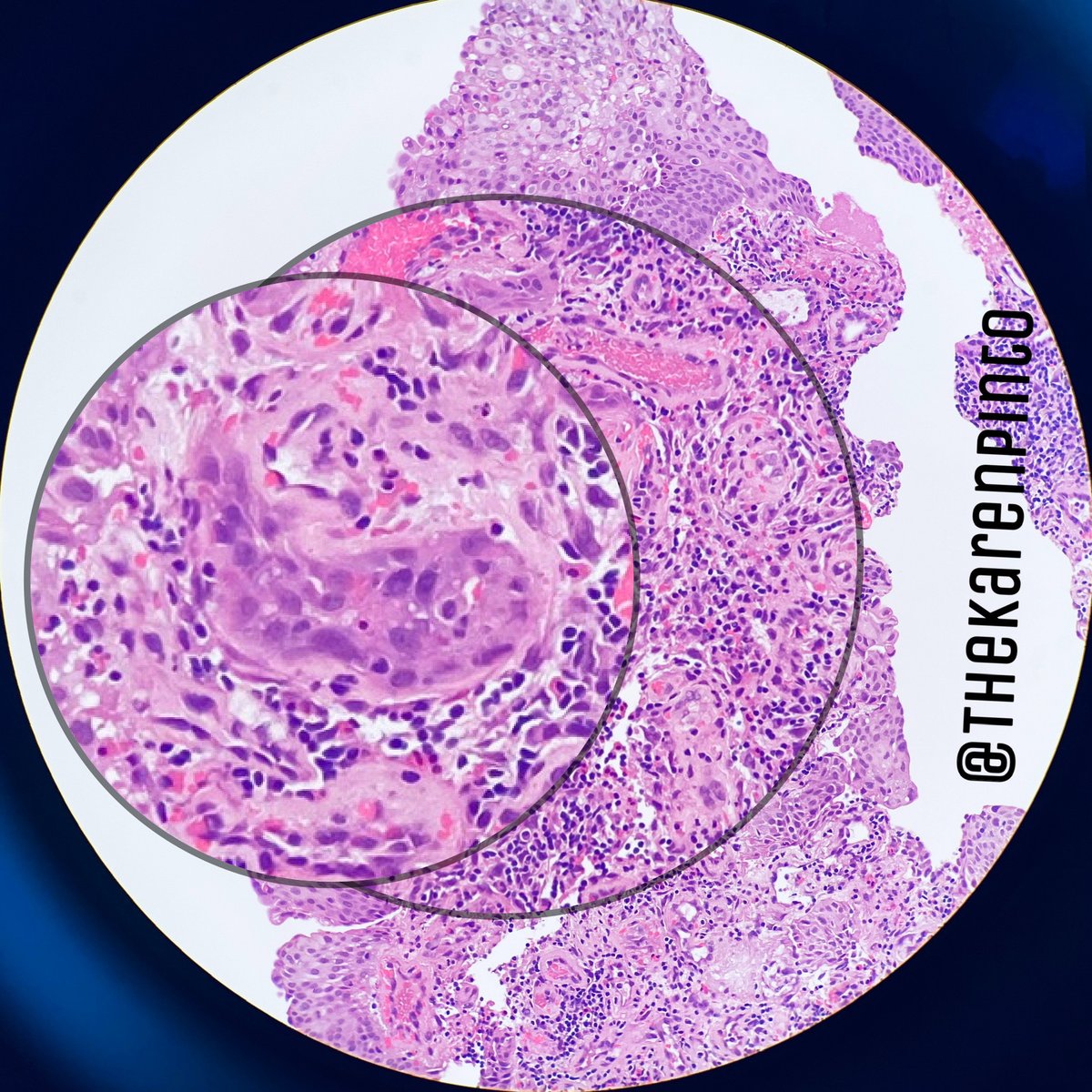
4. Beware of the “invasive” appearing urothelial nests. They are characteristically seen “wrapping around blood vessels with fibrin”




They are NOT invasive (it’s pseudo)
The proliferating epithelium invaginates into the subepithelium, traps the stroma - giving it an invasive look
“Pseudocarcinomatous epithelial hyperplasia”
The proliferating epithelium invaginates into the subepithelium, traps the stroma - giving it an invasive look
“Pseudocarcinomatous epithelial hyperplasia”


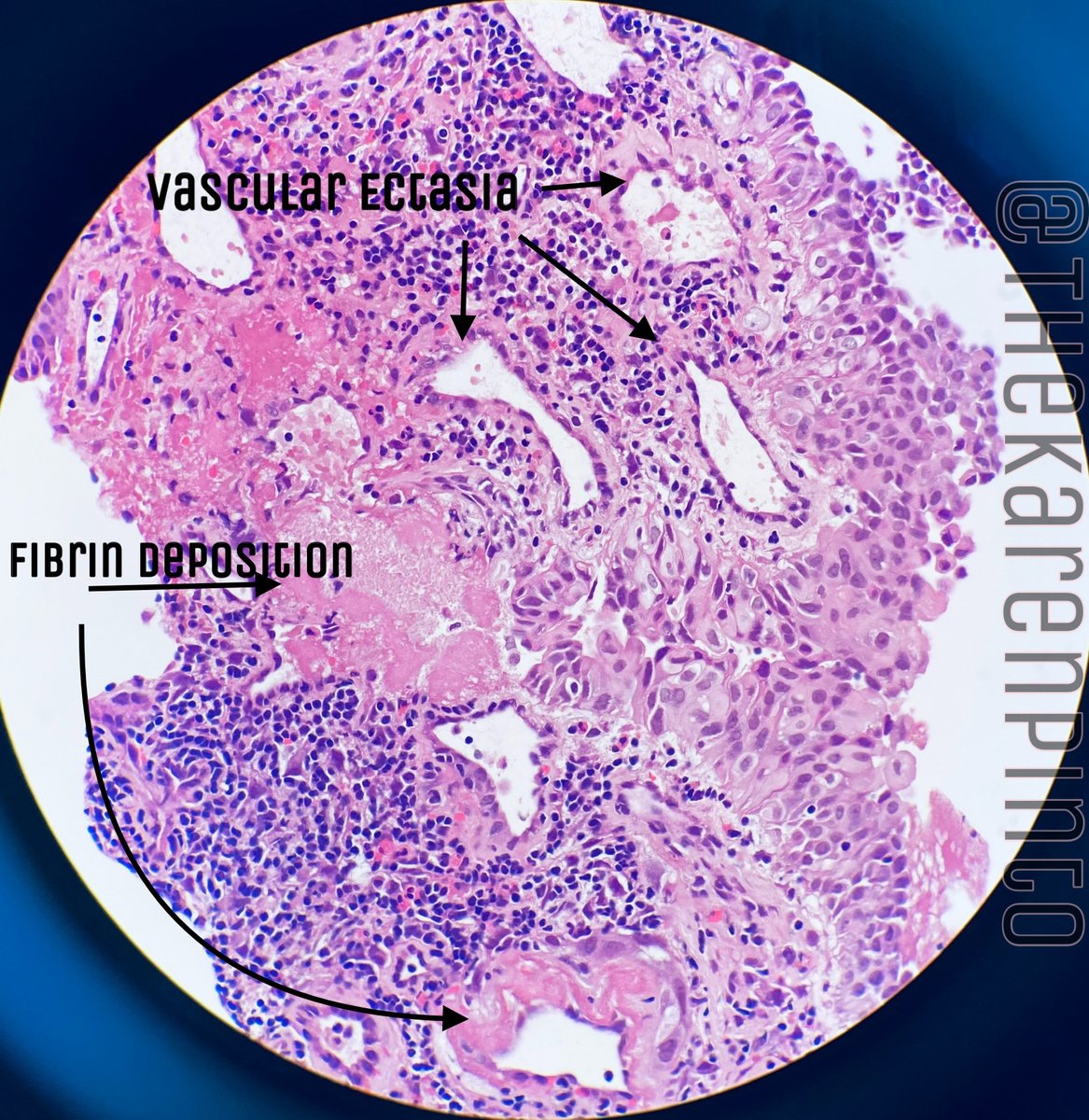
CLUE 2: BLOOD VESSELS:
1. They will be dilated (ectatic)
2. Fibrin deposition +
3. Prominent endothelial cells +
1. They will be dilated (ectatic)
2. Fibrin deposition +
3. Prominent endothelial cells +


CLUE 3: STROMA:
1. Hemorrhage +
2. Weird atypical fibroblasts +
3. Edema
4. Mixed inflammation
5. Collagen deposition
1. Hemorrhage +
2. Weird atypical fibroblasts +
3. Edema
4. Mixed inflammation
5. Collagen deposition




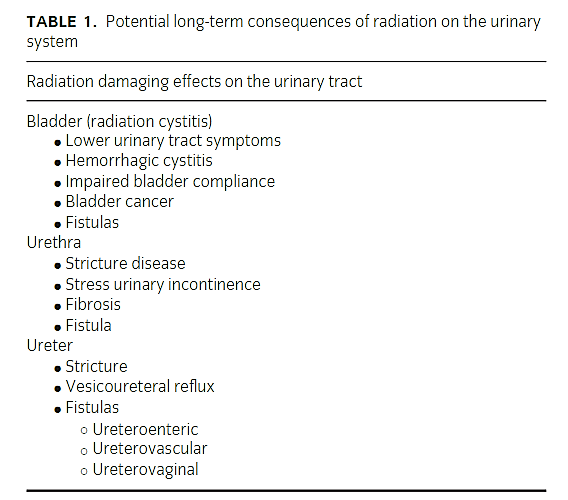
Did you know, there is scale assessing the complications post radiation
IC: Barua SK et al. Int J Adv Med. 2019 Jun;6(3):599-604
IC: Barua SK et al. Int J Adv Med. 2019 Jun;6(3):599-604

Long term complications usually arise due to obliterative endarteritis.
Bladder mucosa necrosis - shed off - hematuria
Permanent dilation of blood vessels - telangiectasia - bleeding
IC: doi.org/10.1111/luts.1…
Bladder mucosa necrosis - shed off - hematuria
Permanent dilation of blood vessels - telangiectasia - bleeding
IC: doi.org/10.1111/luts.1…
Remember:
H&E sometimes can look very frightening and it’s tough to distinguish it from carcinoma.
-Make sure you have the correct history + radiology
-Don’t be over-enthusiastic in calling anything “cancer” for a patient who has received radiation
End of #PathTweetorial
H&E sometimes can look very frightening and it’s tough to distinguish it from carcinoma.
-Make sure you have the correct history + radiology
-Don’t be over-enthusiastic in calling anything “cancer” for a patient who has received radiation
End of #PathTweetorial

