
It’s been over 2 months since the first descriptions of cardiac manifestations of Covid-19. There have been many papers and reviews on this topic. What have we learned about how SARS-CoV-2 can affect the heart? #whyCMR #cardiotwitter
Troponin elevations and low EFs are frequently described. Why do they happen? Most papers use the term Covid-19 myocarditis. But can SARS-CoV-2 cause fulminant myocarditis (= extensive focal myocardial necrosis, as seen with viral lymphocytic or giant cell myocarditis)?
I tried looking at published CMR images and autopsy studies to get some insights into what happens in the hearts of Covid-19 patients. I’ll share my thoughts on 10 papers with CMR images and 2 papers each with autopsy data in >10 patients:
CMR paper 1 – Inciardi RM et al.
DOI – 10.1001/jamacardio.2020.1096
Age – 53
Sex – F
Troponin – 0.89 ng/mL
LVEF – 35% -> 44% (echo)
LGE – Diffuse biventricular
T1 – Not mentioned
T2 – Elevated
Cardiac pathology – None
DOI – 10.1001/jamacardio.2020.1096
Age – 53
Sex – F
Troponin – 0.89 ng/mL
LVEF – 35% -> 44% (echo)
LGE – Diffuse biventricular
T1 – Not mentioned
T2 – Elevated
Cardiac pathology – None

My thoughts on CMR paper 1 – The LGE images are practically uninterpretable. The LVEF recovery, low troponins, etc. don’t fit into fulminant myocarditis.
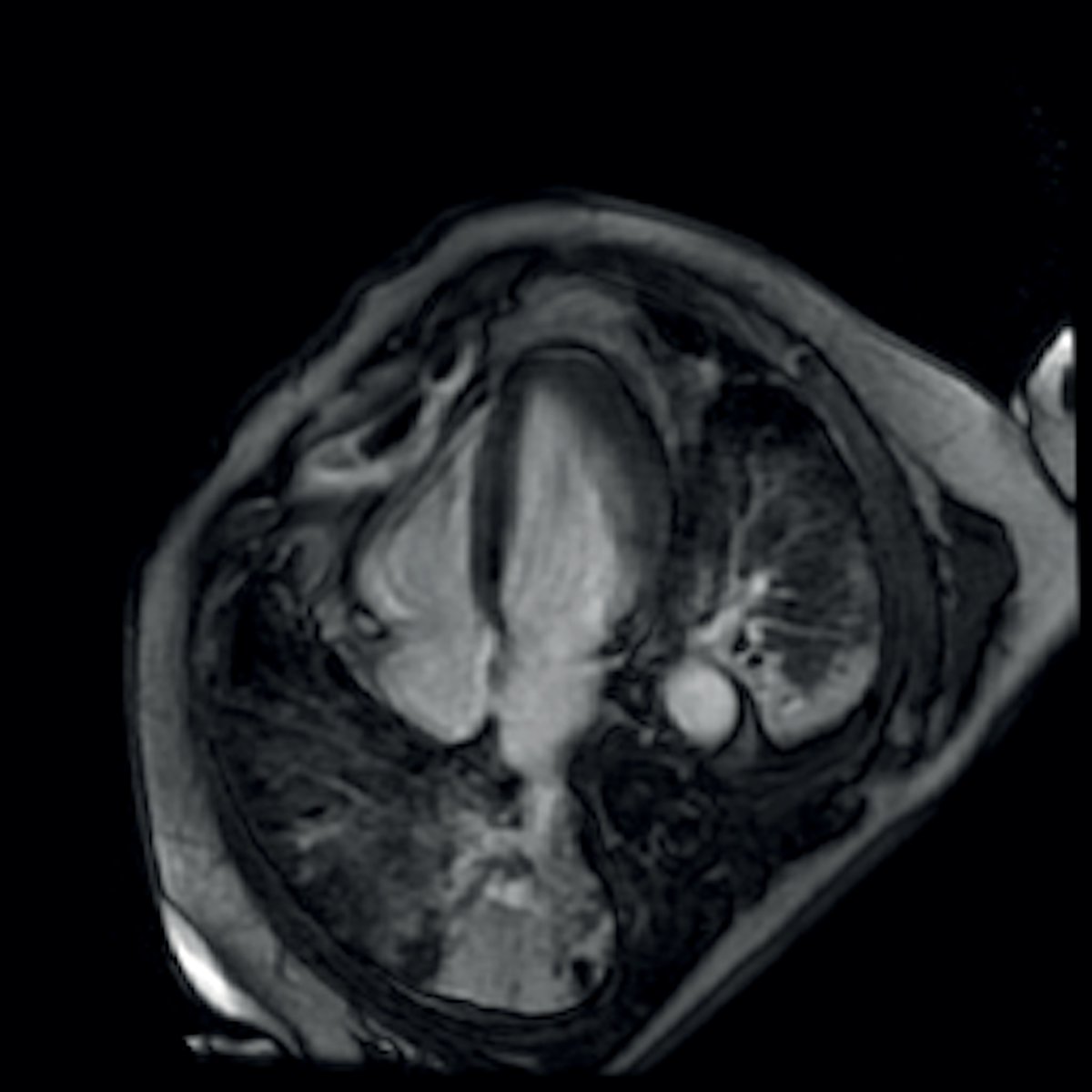
CMR paper 2 – Yuan WF et al.
DOI – 10.21037/cdt.2020.03.08
Age – 33
Sex – M
Troponin – Not mentioned
LVEF – Slightly decreased
LGE – None
T1 – Not mentioned
T2 – Elevated
Cardiac pathology – None
DOI – 10.21037/cdt.2020.03.08
Age – 33
Sex – M
Troponin – Not mentioned
LVEF – Slightly decreased
LGE – None
T1 – Not mentioned
T2 – Elevated
Cardiac pathology – None
My thoughts CMR paper 2 – The isolated T2 abnormality is not convincing; it could very well be an artifact.
CMR paper 3 – Sala S et al.
DOI – 10.1093/eurheartj/ehaa286
Age – 43
Sex – F
Troponin – 135 ng/L
LVEF – 64%
LGE – None
T1 – Elevated
T2 – Elevated
Cardiac pathology – Diffuse T-lymphocytic infiltrates, edema, limited necrosis. No SARS-CoV-2 genome in the myocardium
DOI – 10.1093/eurheartj/ehaa286
Age – 43
Sex – F
Troponin – 135 ng/L
LVEF – 64%
LGE – None
T1 – Elevated
T2 – Elevated
Cardiac pathology – Diffuse T-lymphocytic infiltrates, edema, limited necrosis. No SARS-CoV-2 genome in the myocardium
My thoughts CMR paper 3 – Overall, the CMR suggests stress cardiomyopathy, but the pathology showed lymphocytic infiltrates.
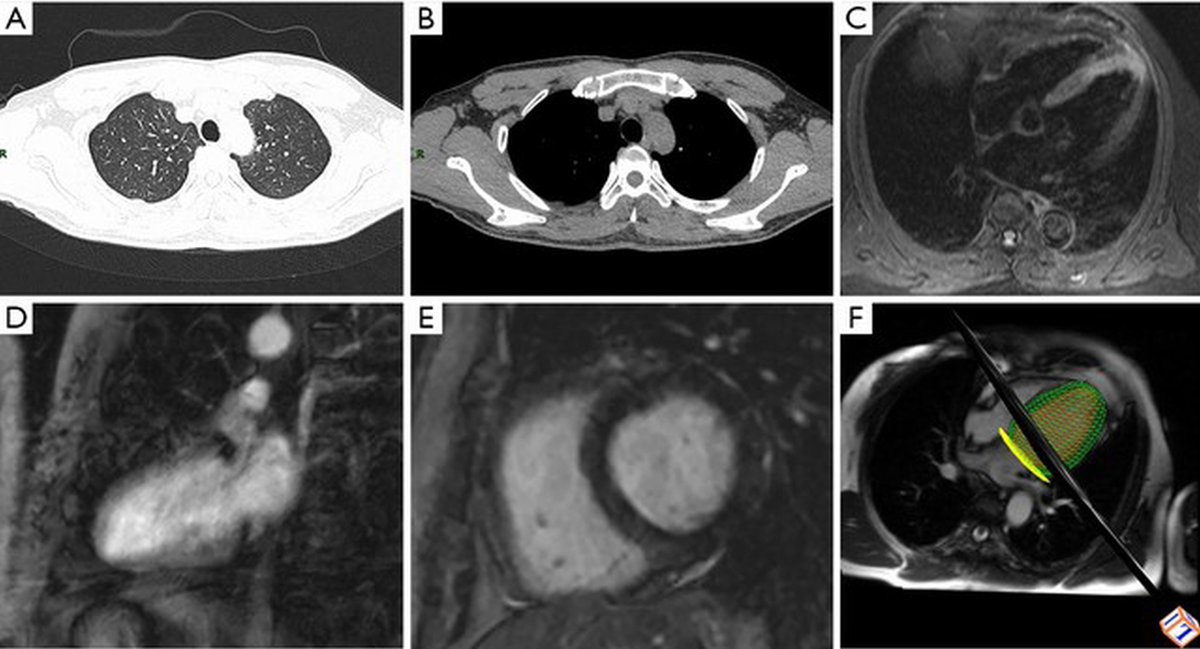
CMR paper 4 – Kim IC et al.
DOI – 10.1093/eurheartj/ehaa288
Age – 21
Sex – F
Troponin – 1.26 mg/mL
LVEF – Severely decreased on echo
LGE – Extensive transmural lateral wall
T1 – Elevated in the lateral wall
T2 – Diffusely elevated in the entire myocardium
Cardiac pathology – None
DOI – 10.1093/eurheartj/ehaa288
Age – 21
Sex – F
Troponin – 1.26 mg/mL
LVEF – Severely decreased on echo
LGE – Extensive transmural lateral wall
T1 – Elevated in the lateral wall
T2 – Diffusely elevated in the entire myocardium
Cardiac pathology – None

My thoughts CMR paper 4 – The LGE is definitely real and the most extensive of all cases here, but not convincing it is acute, based on the T2 (diffuse elevation) and minimal troponin elevation.
CMR paper 5 – Doyen D et al.
DOI – 10.1016/S0140-6736(20)30912-0
Age – 69
Sex – M
Troponin – 9002 ng/L
LVEF – Normal on echo
LGE – Subepicardial in the inferolateral wall and apex
T1 – Not mentioned
T2 – Not mentioned
Cardiac pathology – None
DOI – 10.1016/S0140-6736(20)30912-0
Age – 69
Sex – M
Troponin – 9002 ng/L
LVEF – Normal on echo
LGE – Subepicardial in the inferolateral wall and apex
T1 – Not mentioned
T2 – Not mentioned
Cardiac pathology – None
My thoughts CMR paper 5 – The LGE is not convincing; the patient also had LVH due to hypertensive cardiomyopathy.
CMR paper 6 – Paul JF et al.
DOI – 10.1093/ehjci/jeaa107
Age – 35
Sex – M
Troponin – 2885 ng/L
LVEF – Normal on echo
LGE – Subepicardial in the inferior and lateral walls
T1 – Not mentioned
T2 – Not mentioned
Cardiac pathology – None
DOI – 10.1093/ehjci/jeaa107
Age – 35
Sex – M
Troponin – 2885 ng/L
LVEF – Normal on echo
LGE – Subepicardial in the inferior and lateral walls
T1 – Not mentioned
T2 – Not mentioned
Cardiac pathology – None

My thoughts CMR paper 6 – The LGE is definitely real, but not convincing it is acute since the walls are not thick, and as pointed out by others previously, the pattern could fit with LGE of genetic cardiomyopathy.
CMR paper 7 – Warchol I et al.
DOI – 10.20452/pamw.15309
Age – 74
Sex – M
Troponin – 102 ng/L (in the setting of VT)
LVEF – 20%
LGE – Subepicardial and near-transmural in the inferior and lateral segments
T1 – Not mentioned
T2 – Negative
Cardiac pathology – None
DOI – 10.20452/pamw.15309
Age – 74
Sex – M
Troponin – 102 ng/L (in the setting of VT)
LVEF – 20%
LGE – Subepicardial and near-transmural in the inferior and lateral segments
T1 – Not mentioned
T2 – Negative
Cardiac pathology – None

My thoughts CMR paper 7 – The LGE is definitely real, but not convincing it is acute because the walls are not thick, the T2 is negative, and the LGE pattern (and arrhythmic presentation) again fit with genetic arrhythmogenic cardiomyopathy.
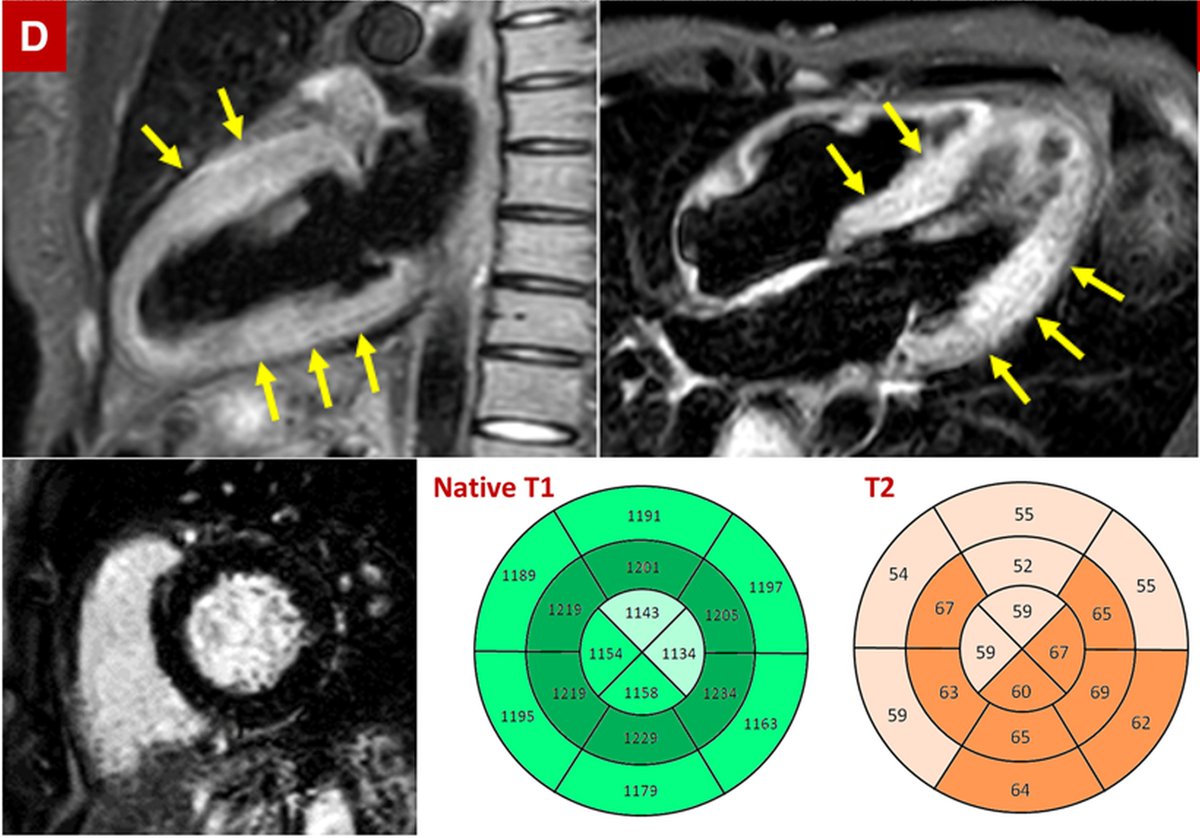
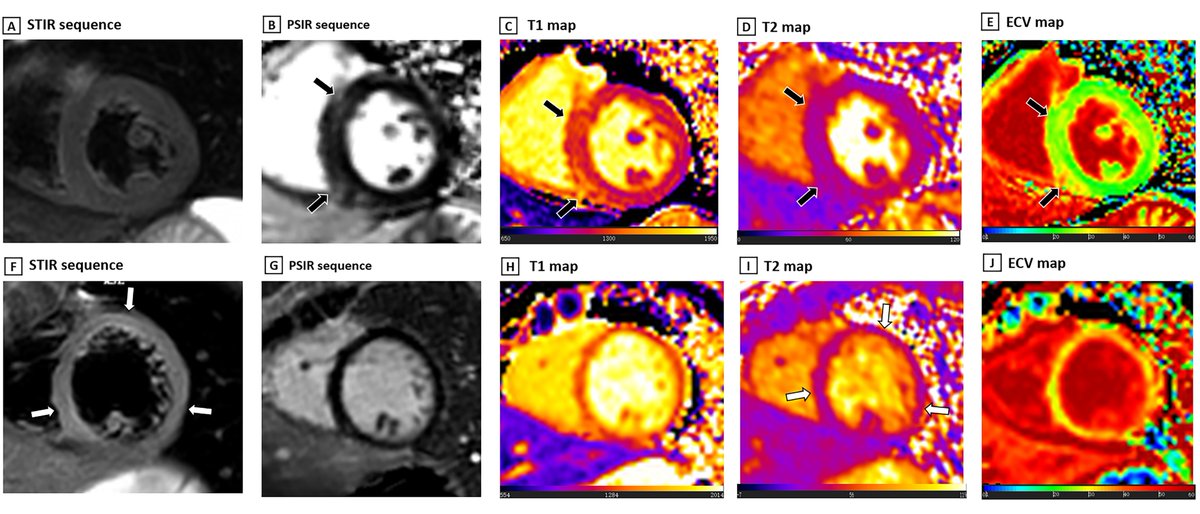
CMR paper 8 – Luetkens JA et al.
DOI – 10.1161/CIRCIMAGING.120.010897
Age – 79
Sex – M
Troponin – 63.5 ng/L
LVEF – 49%
LGE – None
T1 – Elevated at 1035 ms (abnormal ≥1000 ms)
T2 – Elevated at 62 ms (abnormal ≥55.9 ms)
Cardiac pathology – None
DOI – 10.1161/CIRCIMAGING.120.010897
Age – 79
Sex – M
Troponin – 63.5 ng/L
LVEF – 49%
LGE – None
T1 – Elevated at 1035 ms (abnormal ≥1000 ms)
T2 – Elevated at 62 ms (abnormal ≥55.9 ms)
Cardiac pathology – None
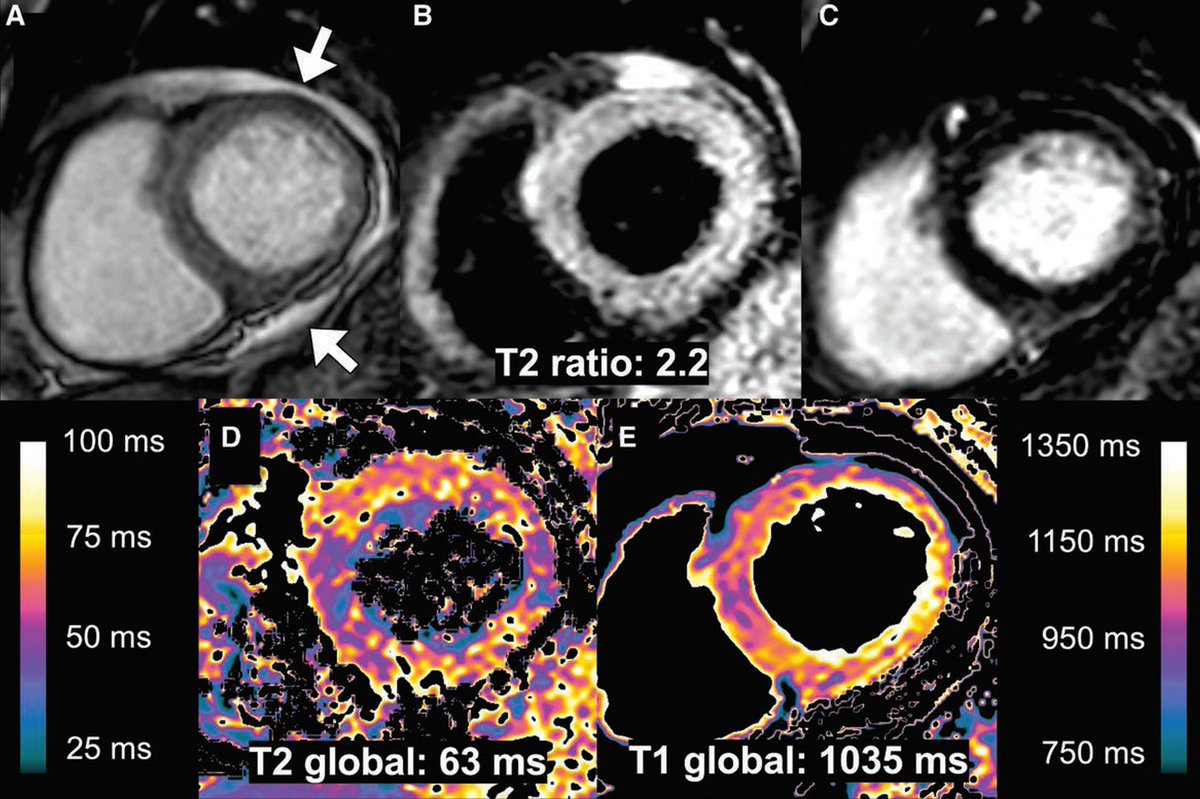
My thoughts CMR paper 8 – Acute inflammation is likely.
CMR paper 9 – Salamanca J et al.
DOI – 10.1016/j.jcmg.2020.05.003
Age – 44
Sex – M
Troponin – 745 ng/L
LVEF – 15% -> 75%
LGE – None
T1 – Elevated at 1120 ms
T2 – Elevated
Cardiac pathology – No inflammatory infiltrates on EMB
DOI – 10.1016/j.jcmg.2020.05.003
Age – 44
Sex – M
Troponin – 745 ng/L
LVEF – 15% -> 75%
LGE – None
T1 – Elevated at 1120 ms
T2 – Elevated
Cardiac pathology – No inflammatory infiltrates on EMB

My thoughts CMR paper 9 – The CMR suggests stress cardiomyopathy.
CMR paper 10 – Huang L et al.
DOI – 10.1016/j.jcmg.2020.05.004
Age – n=26; median 38 y
Sex – 10 M, 16 F
Troponin – Median 2.2 pg/mL (13/26)
LVEF – 60.7% in abnormal CMR
LGE – Present in 8/26
T1 – Elevated at 1271 ms in abnormal CMR
T2 – Elevated in 14/26
Cardiac pathology – None
DOI – 10.1016/j.jcmg.2020.05.004
Age – n=26; median 38 y
Sex – 10 M, 16 F
Troponin – Median 2.2 pg/mL (13/26)
LVEF – 60.7% in abnormal CMR
LGE – Present in 8/26
T1 – Elevated at 1271 ms in abnormal CMR
T2 – Elevated in 14/26
Cardiac pathology – None

My thoughts CMR paper 10 – This is the only paper with >1 case, but the LGE in the Figures is small in extent and not convincing; some of it may possibly be artifacts.
Autopsy paper 1 - Wichmann D et al.
DOI - 10.7326/M20-2003
Number of deceased patients – 12
Cardiac findings – Lymphocytic myocarditis only in the RV in 1 case, preexisting pathology in all cases except 1, viral RNA in the heart in 5 patients.
DOI - 10.7326/M20-2003
Number of deceased patients – 12
Cardiac findings – Lymphocytic myocarditis only in the RV in 1 case, preexisting pathology in all cases except 1, viral RNA in the heart in 5 patients.
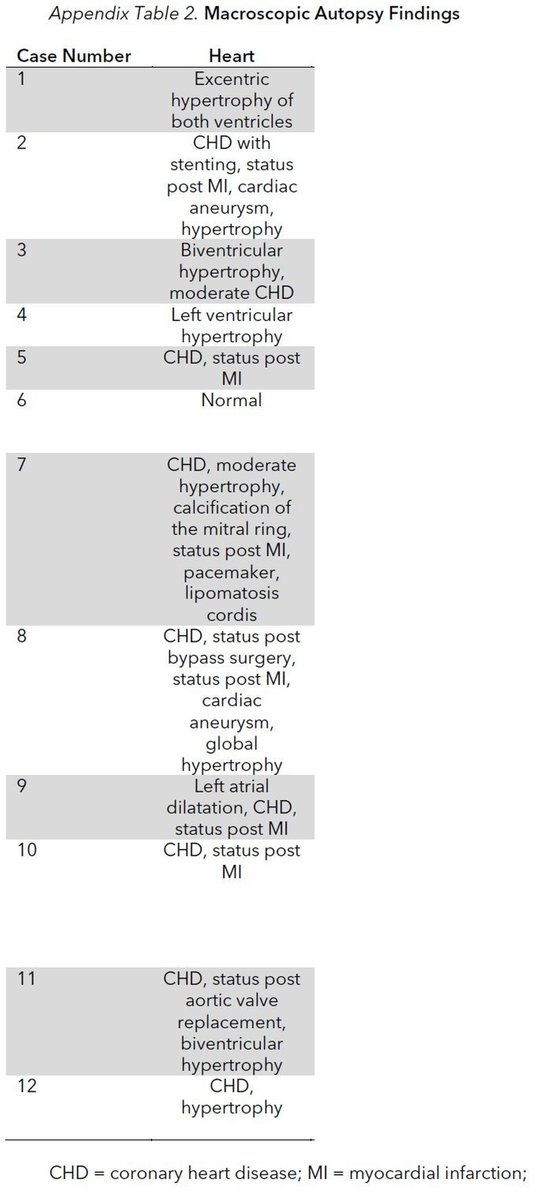
Autopsy paper 2 – Menter T et al.
DOI - 10.1111/his.14134
Number of deceased patients – 21
Cardiac findings – Myocardial hypertrophy in 15, senile cardiac amyloidosis in 6, acute MI in 1, peracute focal myocardial necrosis as a sequela of shock in 3.
DOI - 10.1111/his.14134
Number of deceased patients – 21
Cardiac findings – Myocardial hypertrophy in 15, senile cardiac amyloidosis in 6, acute MI in 1, peracute focal myocardial necrosis as a sequela of shock in 3.

My concluding thoughts: Myocardial inflammation, elevated troponin, and low EF are all possible, but I don't see much convincing evidence that SARS-CoV-2 can directly cause fulminant myocarditis (with extensive necrosis, as in other viral lymphocytic or giant cell myocarditis).
As proposed by others, the myocardial inflammation and reduced EF in some patients may be a response to a cytokine storm and, simply a part of widespread systemic inflammation.
Other pre-existing cardiac diseases could be present in Covid-19 patients and complicate clinical and imaging findings.




