1/ THREAD: Many thanks to all who voted and commented. The better we understand the virus, the better we can protect people. Science matters. Let’s dive into this hard, important question.
2/ OK, if you just want to know the bottom line, you can stop here: no one knows the answer yet. But, if you’re interested to know what we’re learning, how we might find out more, and why it matters, please read on.
3/ Some commenters expressed frustration that we don’t know more. Unfortunately, that’s the nature of science. We learn more every day, but discoveries and breakthroughs take time.
4/ Let’s take the first choice—amount of virus. This is called the inoculum. If you sneeze in my face, there could be an enormous amount of virus. But if I touch a doorknob that has a small residual amount of virus, there might be much, much less. 

5/ There’s actually some evidence to support this hypothesis. Remember the alert doctor Li Wenliang? He was one of the first to report the outbreak, was disciplined by the local government in Wuhan, caught the virus, and, tragically, died from it. bit.ly/2TdOovB
6/ Dr. Li was an ophthalmologist. One theory is that close contact with his patients might have resulted in a large amount of viral exposure. @statnews explains here: bit.ly/2LHtQYr
7/ My sub-sub-sub specialty is tuberculosis. One theory is that the quantity of TB bacteria inhaled is an important factor to how likely we are to get very sick. Another theory suggests a single infectious tubercle bacillus results in infection, and dose isn’t important.
8/ We actually don’t know if inoculum is important for diseases we’ve studied for decades (such as flu) or more than a century (such as tuberculosis). So, it’s no surprise we’re not sure about the inoculum theory—we’re still learning about it for other diseases, too.
9/ It might be possible to study this and to know more from meticulous epidemiological studies of outbreaks and of contacts. But I’m with the majority here—and with these experts. It’s probably not the leading reason for the dramatic differences. bit.ly/2ZeJ8fd
10/ So that brings us to the next possibility: Human genetics. Are some people getting worse disease because of their genetic predisposition?
11/ One theory revolves around a receptor in the lung called ACE2. ACE2 receptors are an important entryway of SAR-CoV-2 (the virus that causes #COVID19) into the lungs. bit.ly/2Tm70d8
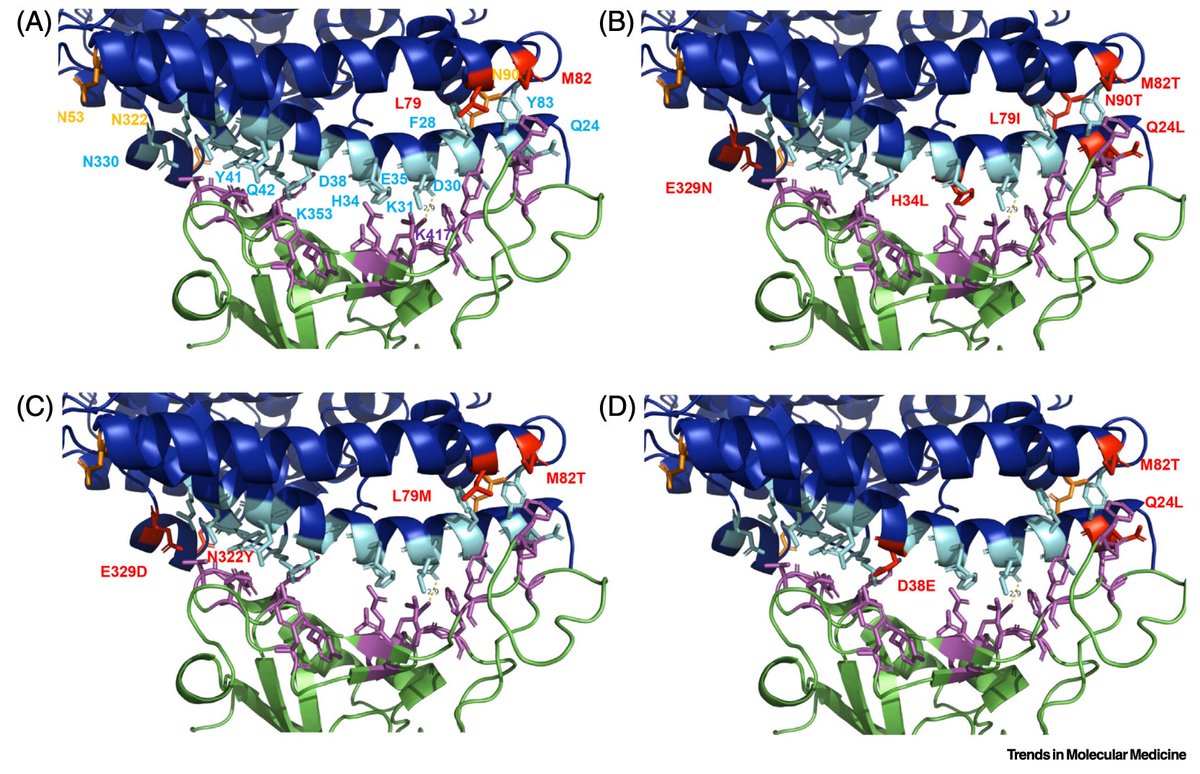
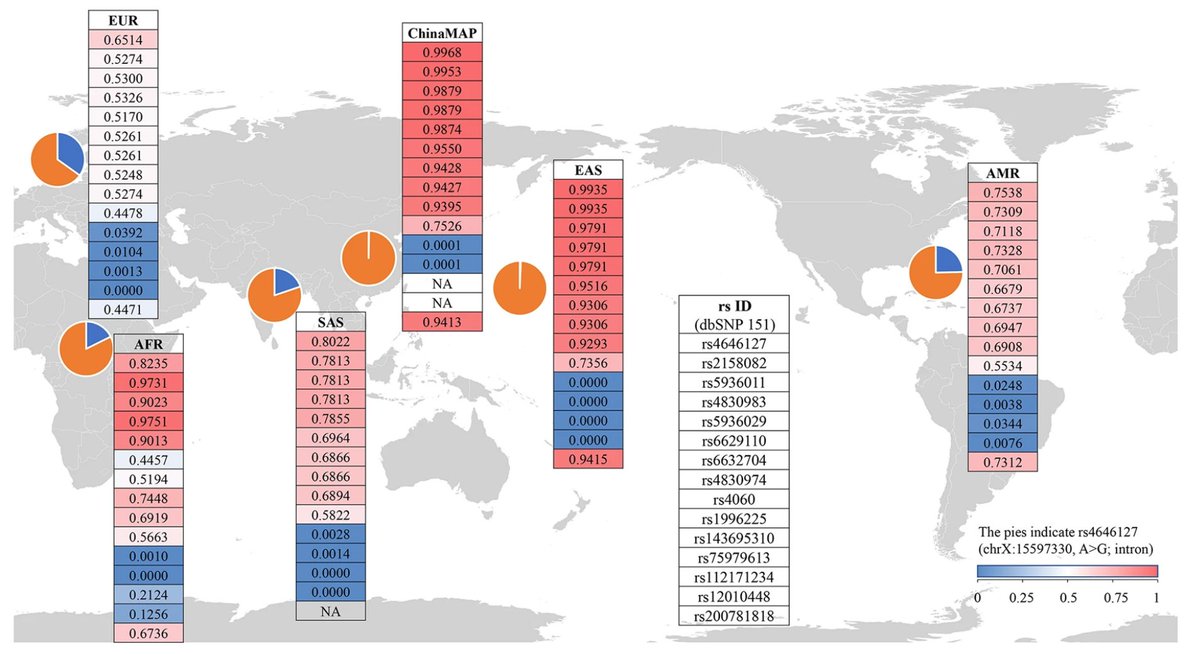
12/ Some people have more receptors than others. In fact, males have more than females, and males with #COVID19 seem to do worse. And maybe children are partly protected because they have less? This study looks at ACE2 variants in different populations: go.nature.com/2z4I1Em
13/ Incidentally, it’s the ACE2 connection that led to concern that certain common antihypertensive medications (known as RAS inhibitors, which include both ACE inhibitors and ARBs) could make patients more susceptible to infection or severe #COVID19.
14/ The great team at @ResolveTSL looked at that early on (Mar. 16) and our assessment has been confirmed by multiple analyses in recent months: there’s no evidence that these medications have an impact on the severity of #COVID19. bit.ly/2yfKACT
15/ There may be other human genetic factors at play besides ACE2 variability, but we’re at the beginning stages of studying these possibilities and really have no idea if human genetics has anything to do with severity of disease.
16/ How about viral genetics? Personally, I think this could be a major source of the variability, but I’m in a minority of public health people studying the virus who think this could be the case.
17/ We know that enveloped RNA viruses—that’s what SAR-CoV-2 is—mutate frequently, as shown in a study on genomic clusters in Victoria, Australia. And we know that the mutations are considered to have been “minor”.
18/ But what we don’t know is whether there is a different level of severity associated with different mutations. Only a study that looks at BOTH genetics and epidemiology can figure that out.
19/ The folks who know this area best tend to doubt this theory, though, and early data from a pre-print from China that suggested there are different types of the virus doesn’t seem to have been replicated.
20/ So, finally, that brings us to human health. Patients who have an underlying condition, such as diabetes, chronic lung disease, or kidney disease are at higher risk of severe illness.
21/ There may be other health factors at play too. It’s tempting to think that Vitamin D deficiency could play a role. fxn.ws/2WMwuT3
22/ Some of the groups that have more severe illness—such as African Americans—also have more vitamin D deficiency. Although it’s possible this could be a factor, it would be unusual to have a single explanation like this of severity.
23/ Many infectious disease specialists suspect that severity has to do with prior infections with other coronaviruses.
24/ Why do kids rarely get severely ill? Is it because they have more recent exposure to similar viruses so they have better immunity? Or do they have less immunity, because they’ve been around for less time?
25/ In the latter theory, immunity makes disease more severe, since more damage comes from the immune reaction than the virus.
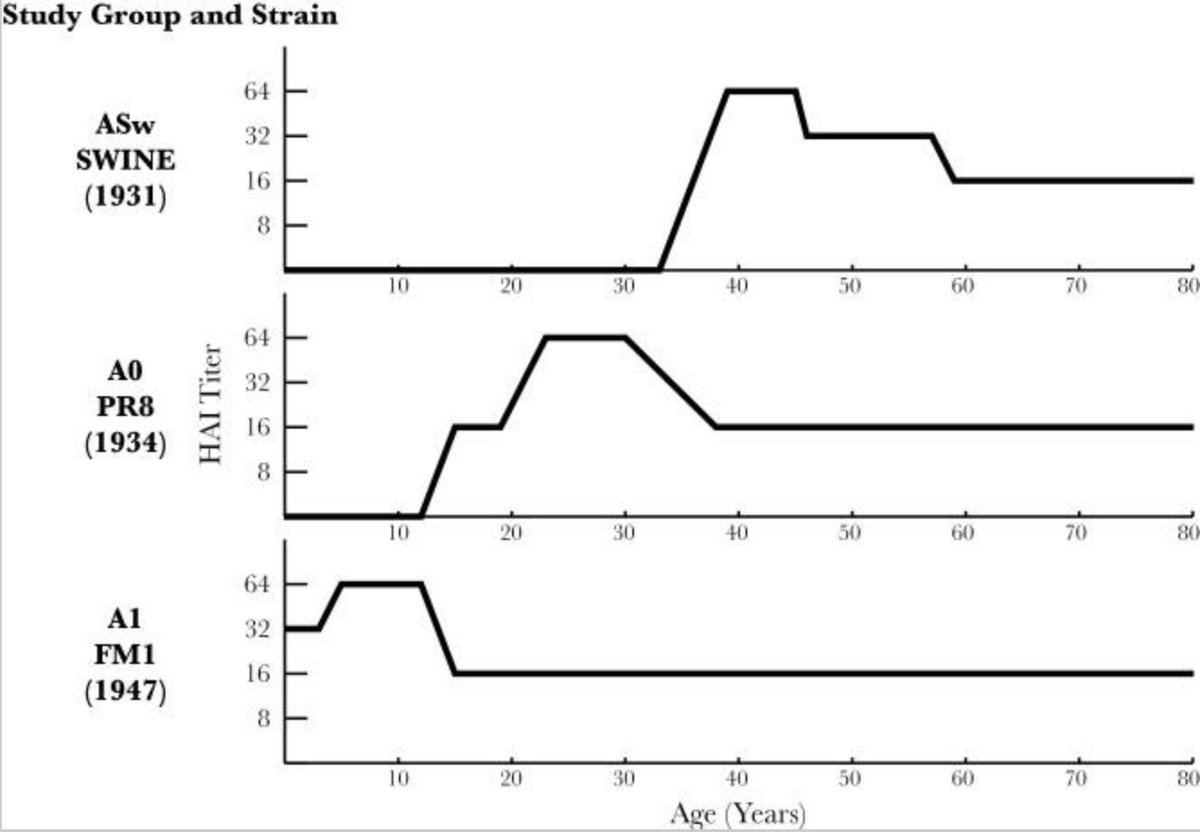
26/ Studies of influenza have found that, in general, whatever strain someone was first infected with becomes the strain they will respond to most effectively. This is called the “original sin” theory of flu immunity imprinting. bit.ly/2WK3uLw
27/ A contrasting new theory about the 1918 pandemic suggests just the opposite: that priming by an earlier infection resulted in MORE severe illness among people who had the earlier infection. bit.ly/2TBQpCn
28/ Bottom line: we have no idea why #COVID19 is more severe in some patients than others. But we do have some theories, and theories should lead to hypotheses, which should lead to investigations (which MUST include both genetics and epidemiology).
29/ Those investigations should lead to more knowledge, which should help us fight the pandemic, including maybe even helping to accelerate development of a vaccine. So, it’s an important question to answer.