1) We’re treating it better:
Needless to say, we’ve learned a lot about the disease since patients flooded ERs in China, Italy and NYC.
We all had patients that we intubated early on that we’d approach differently now.
We’re doing more proning.
There’s even a few treatments!
Needless to say, we’ve learned a lot about the disease since patients flooded ERs in China, Italy and NYC.
We all had patients that we intubated early on that we’d approach differently now.
We’re doing more proning.
There’s even a few treatments!
So maybe just fewer people with severe #COVID19 are dying because us medical professionals have gotten wise and we have better tricks and treatments you our sleeve!
I suspect that’s probably part of it.
How much? Don’t know.
I suspect that’s probably part of it.
How much? Don’t know.

We know that the recent spike in case counts is largely driven by infections in younger age groups (20s-40s).
“In Arizona...people ages 20 to 44 account for nearly half of all cases.”
nytimes.com/2020/06/25/us/…
“In Arizona...people ages 20 to 44 account for nearly half of all cases.”
nytimes.com/2020/06/25/us/…
And “in Florida, the median age of residents testing positive for the virus has dropped to 35, down from 65 in March.”
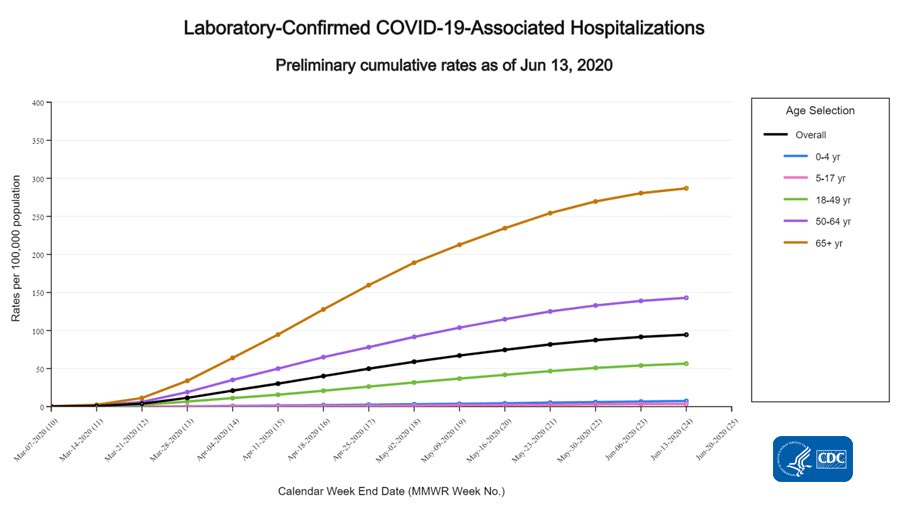
We know younger people are less likely to be hospitalized for #COVID19.
But the worry is they will go on to infect older and more vulnerable groups.
We know younger people are less likely to be hospitalized for #COVID19.
But the worry is they will go on to infect older and more vulnerable groups.
3) The Lag
Deaths are a ‘lagging indicator’. That means you won’t see an increase in deaths from #COVID19 for weeks after an increase in cases. Why?
Exposed ➡️ Sick ➡️ Hospitalized ➡️ Segere Illness ➡️ Intubation ➡️ Death
Each step takes time. Usually 2-4 weeks total.
Deaths are a ‘lagging indicator’. That means you won’t see an increase in deaths from #COVID19 for weeks after an increase in cases. Why?
Exposed ➡️ Sick ➡️ Hospitalized ➡️ Segere Illness ➡️ Intubation ➡️ Death
Each step takes time. Usually 2-4 weeks total.
I made this gif to show how deaths lagged behind cases in NYC. It’s not perfect - our testing and data early on weren’t great, but you get the point.
Ok, so which one of these explains why we’ve had record high cases but our deaths have been dropping?
🤷♂️
It’s likely a mix. We just don’t know yet.
I’ve also seen some theories that the virus has become less lethal, and maybe that explains it? Doubt it.
🤷♂️
It’s likely a mix. We just don’t know yet.
I’ve also seen some theories that the virus has become less lethal, and maybe that explains it? Doubt it.
What do I think will happen???
After this dramatic decline, deaths will undoubtedly rise.
Them crazy youngins will go on to infect their parents and grandma.
And the lag will eventually catch up with us.
Yet our ERs and ICUs are arguably better prepared than we were in NYC...
After this dramatic decline, deaths will undoubtedly rise.
Them crazy youngins will go on to infect their parents and grandma.
And the lag will eventually catch up with us.
Yet our ERs and ICUs are arguably better prepared than we were in NYC...
They’ve got more in their arsenal to treat these patients and hopefully that’ll help prevent some of the #COVID19 deaths.
We will just have to wait, and hope for the best. 🤞
But setting record high case counts on a daily basis will certainly lead to more deaths. Guaranteed.
We will just have to wait, and hope for the best. 🤞
But setting record high case counts on a daily basis will certainly lead to more deaths. Guaranteed.
Lastly, an important reminder that it isn’t just about deaths.
I survived Ebola, a disease well-known to cause a host of chronic & debilitating symptoms.
And recently @edyong209 has reminded us that #COVID19 might leave a same sad toll on its survivors.
theatlantic.com/health/archive…
I survived Ebola, a disease well-known to cause a host of chronic & debilitating symptoms.
And recently @edyong209 has reminded us that #COVID19 might leave a same sad toll on its survivors.
theatlantic.com/health/archive…
Most lastly, I blame the multiple grammatical errors and typos in this thread on the fact that I was completely sober while composing it.