
The kidneys in essence have 3 functions:
1. Glomerular function = Clearance
2. Tubular function = Homeostasis
3. Neurohumoral function
GFR mainly reflects 1. So why do we take GFR (or its estimate Cr) as a surrogate for renal function?
1. Glomerular function = Clearance
2. Tubular function = Homeostasis
3. Neurohumoral function
GFR mainly reflects 1. So why do we take GFR (or its estimate Cr) as a surrogate for renal function?
Look at GFR determinants (=N x snGFR).
In stable circumstances, GFR mainly reflects the number of functional nephrons.
Starting from 1 million per kidney at birth, one loses 5,000-10,000 per year with aging: age-related GFR decline <1 mL/min/1.73m²/y
ncbi.nlm.nih.gov/pmc/articles/P…
In stable circumstances, GFR mainly reflects the number of functional nephrons.
Starting from 1 million per kidney at birth, one loses 5,000-10,000 per year with aging: age-related GFR decline <1 mL/min/1.73m²/y
ncbi.nlm.nih.gov/pmc/articles/P…
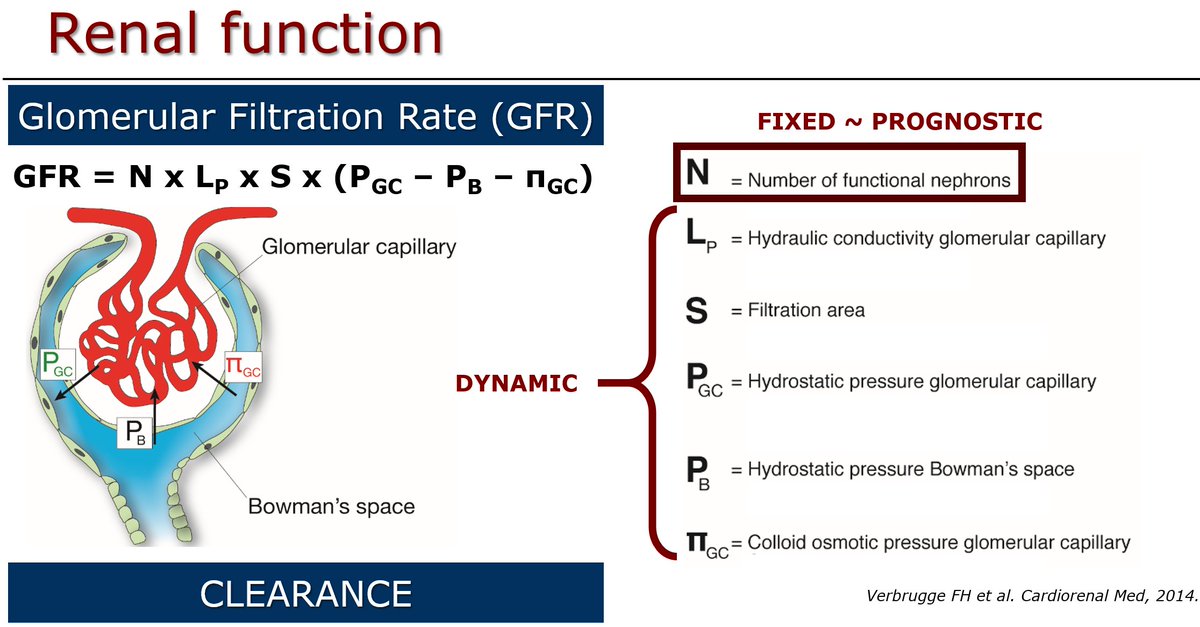
Degree of CKD ~ 1/N: prognostic! Or otherwise, more functional nephrons equals better kidney function.
If you are a nephrologist, it thus makes sense to follow GFR over time as a surrogate for N & degree of #CKD.
But, this assumes that single-nephron GFR remains stable!
If you are a nephrologist, it thus makes sense to follow GFR over time as a surrogate for N & degree of #CKD.
But, this assumes that single-nephron GFR remains stable!
This is why KDIGO classification for CKD incorporates (micro-)albuminuria as well, as a surrogate for snGFR.
In conditions where snGFR⬆️(albuminuria/proteinuria): GFR overestimates the number of functionally intact nephrons. CKD is thus more severe!
In conditions where snGFR⬆️(albuminuria/proteinuria): GFR overestimates the number of functionally intact nephrons. CKD is thus more severe!
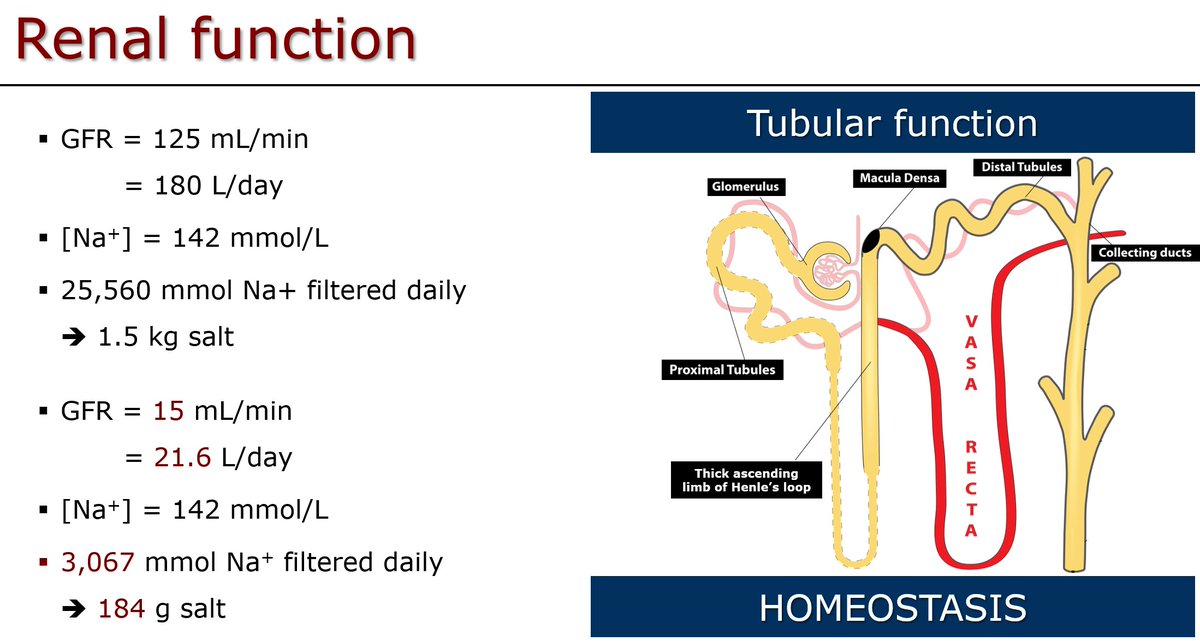
Biggest problem in #ICU is often homeostasis (volume, electrolytes) rather than clearance (uremia).
Remember, homeostasis is mostly a tubular rather than glomerular function. Even with GFR 15 mL/min, one filters >20 L & 184 g salt per day! More than enough to get rid of those!
Remember, homeostasis is mostly a tubular rather than glomerular function. Even with GFR 15 mL/min, one filters >20 L & 184 g salt per day! More than enough to get rid of those!
That's why I am not so worried at ICU if Cr rises, but urine output remains preserved!
Actually, I don't care about Cr too much at all & do not try to prevent a rise. Instead, I'll try to keep good perfusion & get rid of congestion. This saves nephrons & kidney on the long run!
Actually, I don't care about Cr too much at all & do not try to prevent a rise. Instead, I'll try to keep good perfusion & get rid of congestion. This saves nephrons & kidney on the long run!

