
So how safe is #Ibrutinib ?
A very relevant question given that it needs to be administered indefinitely.
41% discontinuation rate in the "real world", most d/t toxicity.
Thread [1/12]
A very relevant question given that it needs to be administered indefinitely.
41% discontinuation rate in the "real world", most d/t toxicity.
Thread [1/12]
So what are the major adverse events anyway ?
1. A fib
2. ⬆️ Risk of bleeding
3. ⬆️ Infections
4. Arthralgias
5. Htn
6. Diarrhoea
7. Pneumonitis
[2/12]
1. A fib
2. ⬆️ Risk of bleeding
3. ⬆️ Infections
4. Arthralgias
5. Htn
6. Diarrhoea
7. Pneumonitis
[2/12]
A very common concern is tox no.1 and 2 .
⬆️A .fib = anticoag for stroke prophylax. but that's when tox no.2 comes into play.
Very difficult to ⚖️ it out .
In RESONATE trial >grade 3 afib in 3% of pts.
Most events occur within 3 mts of starting #ibrutinib
[3/12]
⬆️A .fib = anticoag for stroke prophylax. but that's when tox no.2 comes into play.
Very difficult to ⚖️ it out .
In RESONATE trial >grade 3 afib in 3% of pts.
Most events occur within 3 mts of starting #ibrutinib
[3/12]
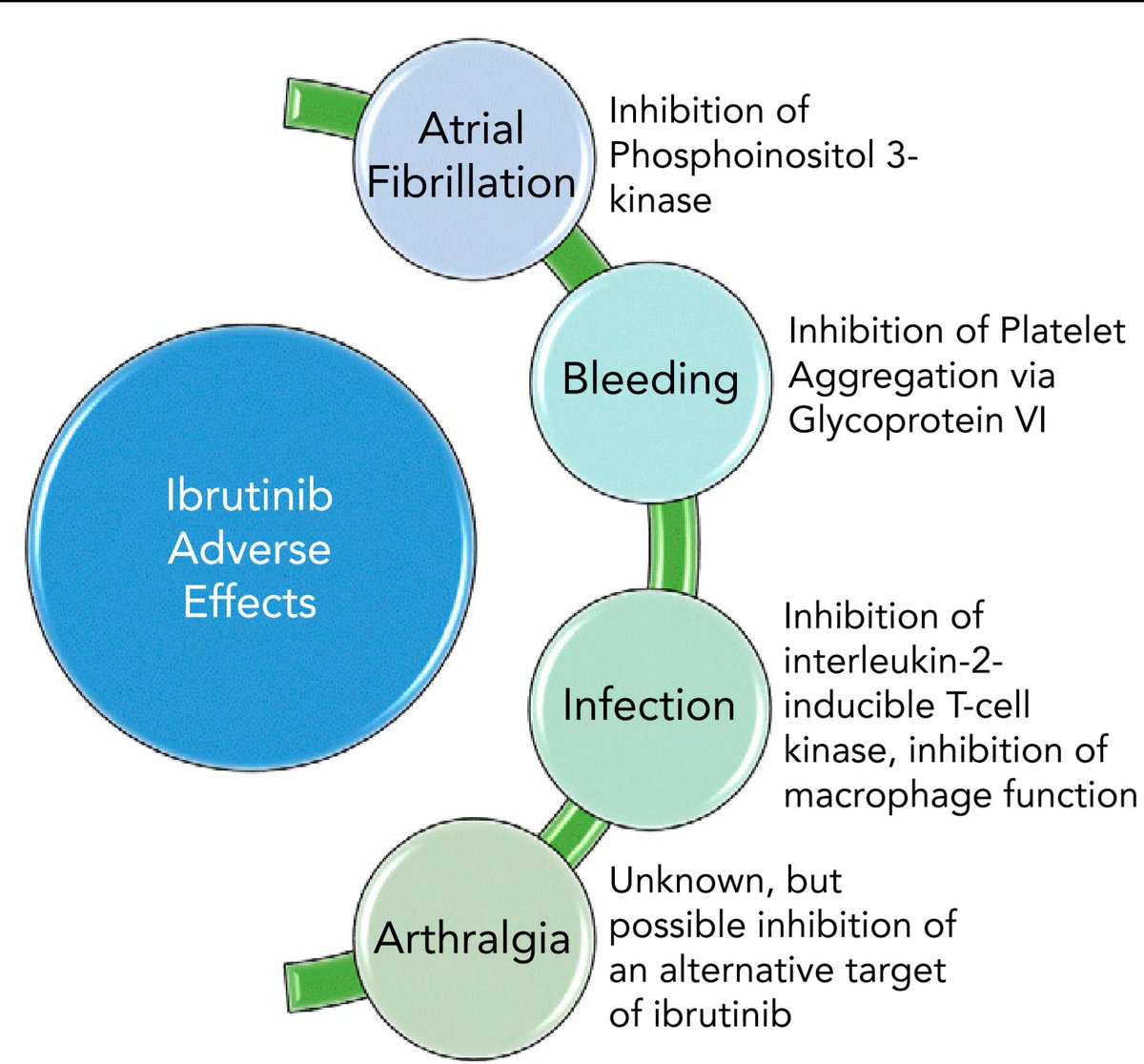
A beautiful image summarising the mechanism of #ibrutinib related ADRs
As we can see most ADRs are d/t off target kinase inhibition.
[4/12]
As we can see most ADRs are d/t off target kinase inhibition.
[4/12]
Talking about bleeds with #ibrutinib .
RESONATE trial : 44% bleeding events, most were minor.
However in the real world setting upto 19% had > grade 3 bleeds.
Concurrent use of anticoag and antiplat agents ⬆️⬆️ risk of major bleeds
[5/12]
RESONATE trial : 44% bleeding events, most were minor.
However in the real world setting upto 19% had > grade 3 bleeds.
Concurrent use of anticoag and antiplat agents ⬆️⬆️ risk of major bleeds
[5/12]
This is a major problem for pts who need anticoag for stroke prophylaxis sec to afib .
Obviously CHA2 DS2 VASc is to be used and anticoag only if score >2.
[6/12]
Obviously CHA2 DS2 VASc is to be used and anticoag only if score >2.
[6/12]
So what anticoag is safe ??
Warfarin ❌
Dabigatran ❌
Rivaroxaban ❌
Apixaban ❌
Off label enoxaparin ✅
Best is to try alternate Rx , W/H #ibrutinib if possible.
[7/12]
Warfarin ❌
Dabigatran ❌
Rivaroxaban ❌
Apixaban ❌
Off label enoxaparin ✅
Best is to try alternate Rx , W/H #ibrutinib if possible.
[7/12]
⬆️ Infections , another massive problem.
Pneumonia➡️Most common
Most worrisome ,Aspergillus Fumigatus IFI.
PcP another cause of concern
RESONATE reported a 24% incidence of >grade 3 infections.
⬇️ Activation of macrophages d/t BTK inhibition l/t ⬆️ A.fumigatus
[8/12]
Pneumonia➡️Most common
Most worrisome ,Aspergillus Fumigatus IFI.
PcP another cause of concern
RESONATE reported a 24% incidence of >grade 3 infections.
⬇️ Activation of macrophages d/t BTK inhibition l/t ⬆️ A.fumigatus
[8/12]
IFI = Azoles , BUT not when using #ibrutinib
Drug interactions ✅
Azoles ⬇️ CYP3a4 = ⬆️ ibrutinib levels
So what does one use ?
AmpB or echinocandins ✅
Problem: no #oral preparation !!
One can use Azoles and #ibrutinib concurrently after ibru dose ⬇️⬇️
140mg ✅
[9/12]
Drug interactions ✅
Azoles ⬇️ CYP3a4 = ⬆️ ibrutinib levels
So what does one use ?
AmpB or echinocandins ✅
Problem: no #oral preparation !!
One can use Azoles and #ibrutinib concurrently after ibru dose ⬇️⬇️
140mg ✅
[9/12]
Diarrhoea d/t EGFR ⛔ is v.common , actually the MC ADR .
But it's fortunately short lived and not very severe.
Loperamide helps.
Another ADR d/t EGFR ⛔ is palpable pruritic rash ,this again is self limited.
Topical steroids help.
[10/12]
But it's fortunately short lived and not very severe.
Loperamide helps.
Another ADR d/t EGFR ⛔ is palpable pruritic rash ,this again is self limited.
Topical steroids help.
[10/12]
Htn is seen in 1/5 pts with only 1/20 having severe HTn .
But this, unlike all other ADRS doesn't ⬇️ with prolonged #ibrutinib Rx .
Rule of thumb :
For any >grade 3 ADR ➡️ W/H #Ibrutinib
Restart at same dose after 1st hold
⬇️ By 1 level after subsequent holds.
[11/12]
But this, unlike all other ADRS doesn't ⬇️ with prolonged #ibrutinib Rx .
Rule of thumb :
For any >grade 3 ADR ➡️ W/H #Ibrutinib
Restart at same dose after 1st hold
⬇️ By 1 level after subsequent holds.
[11/12]
Try alternate Rx if frequent drug holds reqd.
Indefinite therapy is a major issue.
Financial toxicity also needs to be addressed especially in 🇮🇳 where the majority are uninsured.
Blood 2019
doi.org/10.1182/blood-…
[12/12]
Indefinite therapy is a major issue.
Financial toxicity also needs to be addressed especially in 🇮🇳 where the majority are uninsured.
Blood 2019
doi.org/10.1182/blood-…
[12/12]

