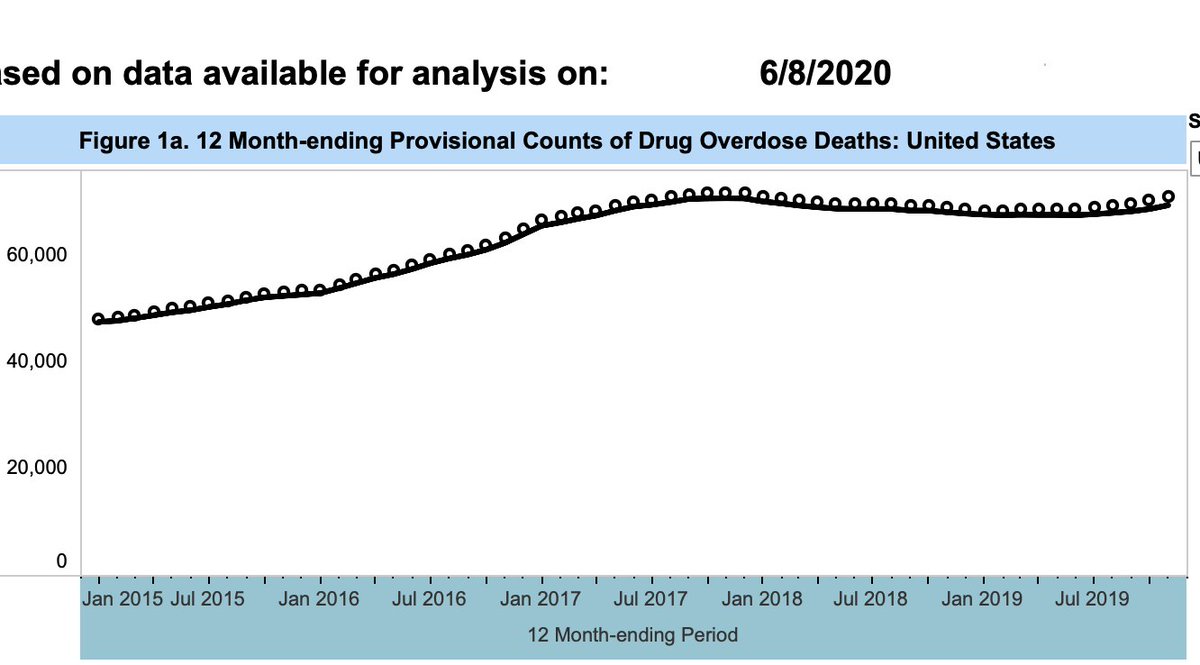
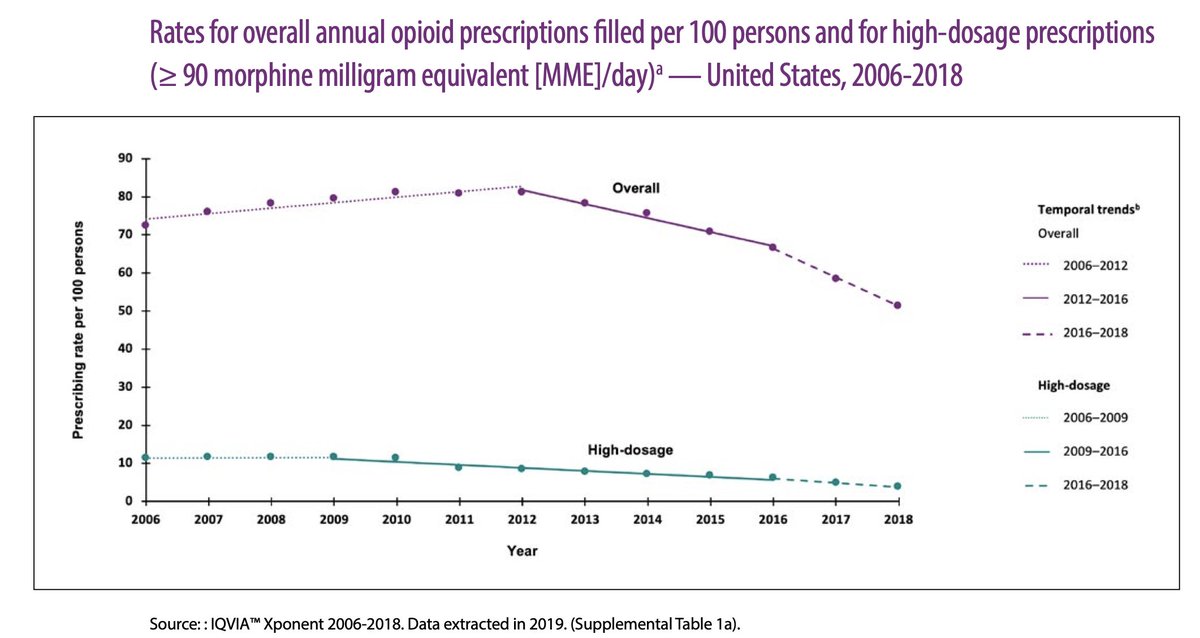
2/Because a rise in #opioid Rx’s contributed to opioid use disorder in the US, public health leaders fixated on pills as “vector of disease” and cutting those Rx’s as the key to solving a crisis. And cut we did: opioid Rx/capita are 19% lower than in 2006. cdc.gov/drugoverdose/p… 
4/The “best case” for Rx opioid taper is that in hands of smart, caring experts (like @drrobbietee, who we salute), motivated patients who were dysfunctional at hi dose regain function as dose comes down slowly, as *part of rehabilitation-minded care*
jamanetwork.com/journals/jamai…
jamanetwork.com/journals/jamai…
5/But rehabilitation-minded care, with consenting patients is an exception. Other experts report *poor* results. They report worse pain in 53% of tapered patients. 36% fled the expert clinic. Driving patients away doesn’t necessarily make them safer. academic.oup.com/painmedicine/a…
6/Other papers find most opioid Rx reduction takes place *fast*,with ⬆️risk of patient death by OD or suicide, ⬆️risk of heroin use*.I’m NOT saying EVERY patient has those outcomes. Don't oversimplify, padawans.
this
journals.plos.org/plosone/articl…
and: bit.ly/2YMg5Pn
this
journals.plos.org/plosone/articl…
and: bit.ly/2YMg5Pn
7/These papers find 4x increased termination of care after opioid taper, and YES: we taper disproportionately on women>men and Blacks>Whites. Why, probably we do our worst to people with less power @DrChinazo
pubmed.ncbi.nlm.nih.gov/31428983/
academic.oup.com/painmedicine/a…
pubmed.ncbi.nlm.nih.gov/31428983/
academic.oup.com/painmedicine/a…

8/With such weak data, it should bother us that thought leaders pushed opioid taper as “the” key to safety. A non-evidence-based view is baked into quality metrics,payment, laws, enforcement by state boards, & criminal investigation thresholds used by HHS: oig.hhs.gov/oei/reports/oe…
9/This system incentivizes patient abandonment. Evidence suggests 40% of primary care docs *won’t accept patients on opioids*. Their metrics for prescribing look EXCELLENT. Up to 10 million patients at risk of being abandoned. A problem? @PoojaLagisetty ncbi.nlm.nih.gov/pmc/articles/P…
10/My @TEDx reviews a *safety* issue without insulting your intelligence. What we DON’T need are smokescreen letters that it’s “been difficult” for “fearful” folks who “believe they are being unfairly penalized”, as one wrote. Dudes, this isn’t a bad movie. This is life & death.
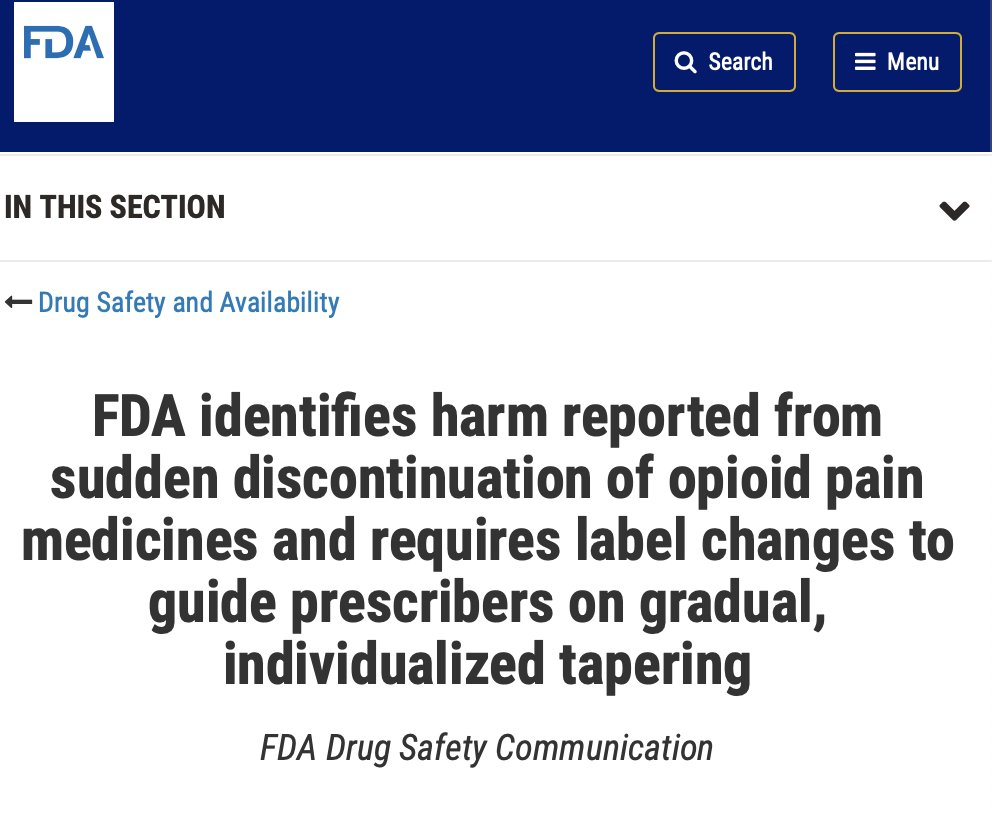
11/The reason 3 federal agencies spoke out in 2019 (CDC, FDA, HHS), was because scientific papers, families & authorities saw ACTUAL harm. And no, we don’t fully understand why such bad things happen, alongside good. Hence the *need for rigorous research* fda.gov/drugs/drug-saf…
12/There is room to debate how WE fix this. My start points are (a)discuss “opioid concerns” as part of a vision for *how we care for people with complex illness*,not just “pro-” or “anti-opioid” & (b include patients & families in policy deliberation without patronizing or pity
13/Note: there is a *chasm* between saying “this would be good care” and making health systems deliver good care. That chasm is filled by “implementation science”. Now is time to take “HOW” we change care as seriously as what we think might be good.cfirguide.org
14/Lastly, let’s pre-rebut some inevitable oversimplifications. Data do not show opioids are magical mannah from heaven, but they can be helpful for some, if you shoulder the downsides. If we had a magic pain treatment that worked for “most” we would offer it. But we do NOT.
15/And yes, I’m very aware of addiction issues, as a front-line internist and addiction scholar. I wrote about opioid Rx’s in 2008, including overprescribing to Whites and undeprescribing to Blacks and Latinx patients with serious pain problems: jamanetwork.com/journals/jama/…
16/Please view & share my @TEDx talk “We Need to Measure the Opioid Crisis Differently”. Let’s make clear that this is a message policy makers, families, patients, and clinicians need to hear.