1/
Was able to join @BIDMC_Medicine Blumgart Firm conf for a fascinating case I had! #IDTwitter #MedTwitter @BIDMC_IDFellows @WendyStead5
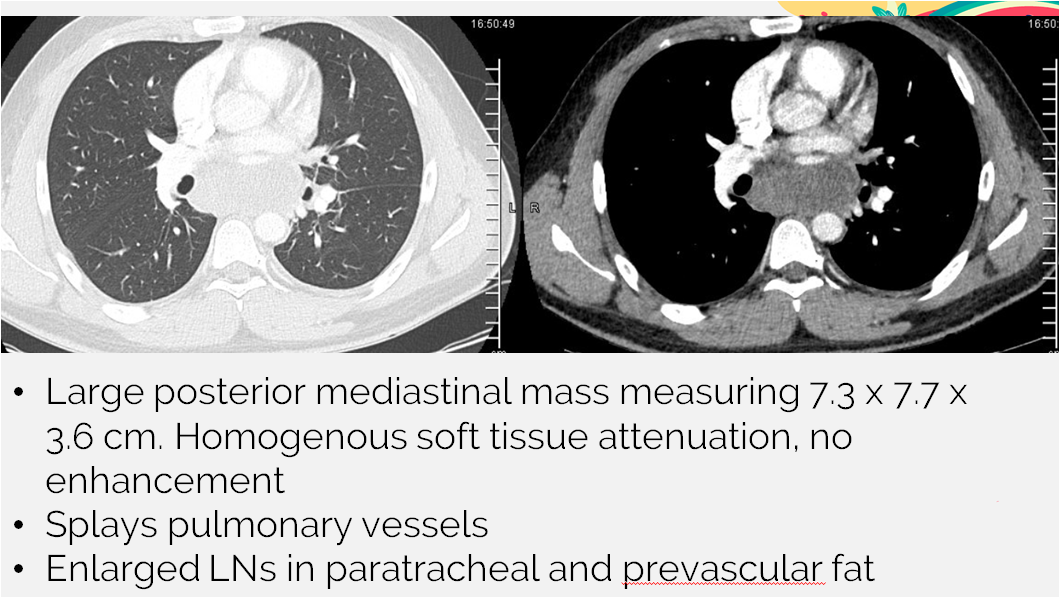
30M w/fever 103, chest tightness that radiates into R neck. CT chest demonstrated a large posterior mediastinal mass with associated LAD 👇
Was able to join @BIDMC_Medicine Blumgart Firm conf for a fascinating case I had! #IDTwitter #MedTwitter @BIDMC_IDFellows @WendyStead5
30M w/fever 103, chest tightness that radiates into R neck. CT chest demonstrated a large posterior mediastinal mass with associated LAD 👇
2/
🔻Goes for bronch/EBUS: frank pus when LNs aspirated. Strep anginosus grew from blood cx + LN tissue cx.
🔻Started on Unasyn with rapid improvement!
🔻Repeat CT chest after ~2 wks of therapy already with decrease to ½ the original size!!!
🔻Goes for bronch/EBUS: frank pus when LNs aspirated. Strep anginosus grew from blood cx + LN tissue cx.
🔻Started on Unasyn with rapid improvement!
🔻Repeat CT chest after ~2 wks of therapy already with decrease to ½ the original size!!!
3/
Let’s talk about the Strep anginosus group!
🦠Formerly S.milleri
🦠Includes S. anginosus, intermedius, constellatus
🦠Viridans strep subgroup
🦠Variable hemolysis but classic = beta-hemolytic pinpoint colonies
🧫Known for butterscotch/caramel odor! (diacetyl production)
Let’s talk about the Strep anginosus group!
🦠Formerly S.milleri
🦠Includes S. anginosus, intermedius, constellatus
🦠Viridans strep subgroup
🦠Variable hemolysis but classic = beta-hemolytic pinpoint colonies
🧫Known for butterscotch/caramel odor! (diacetyl production)
4/
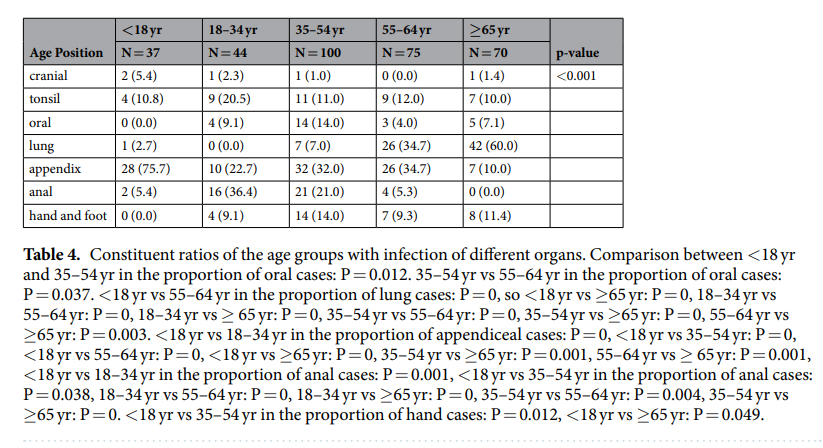
👶🧑🧓Infections noted across the age spectrum
👉nature.com/articles/s4159…
This study looked at 462 pts ranging from 6 mo to 103 yo! Highest incidence was 35-54 yo
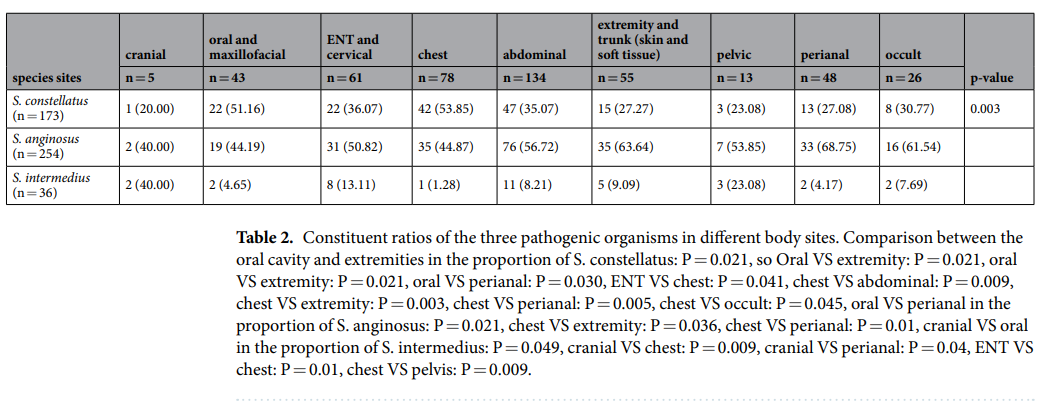
👉Variety of sites of infection (see below) - will talk a little more on that later
👶🧑🧓Infections noted across the age spectrum
👉nature.com/articles/s4159…
This study looked at 462 pts ranging from 6 mo to 103 yo! Highest incidence was 35-54 yo
👉Variety of sites of infection (see below) - will talk a little more on that later
5/
🚨Known for propensity to form abscesses!!🚨
🎈Virulence factors not fully understood
🎈Mixed infections with oral or GI orgs can contribute to abscess➡️think about anaerobes along for the ride, such as Fusobacterium nucleatum
🚨Known for propensity to form abscesses!!🚨
🎈Virulence factors not fully understood
🎈Mixed infections with oral or GI orgs can contribute to abscess➡️think about anaerobes along for the ride, such as Fusobacterium nucleatum
6/
~¾ S.anginosus infections = polymicrobial
👉pubmed.ncbi.nlm.nih.gov/29050796/
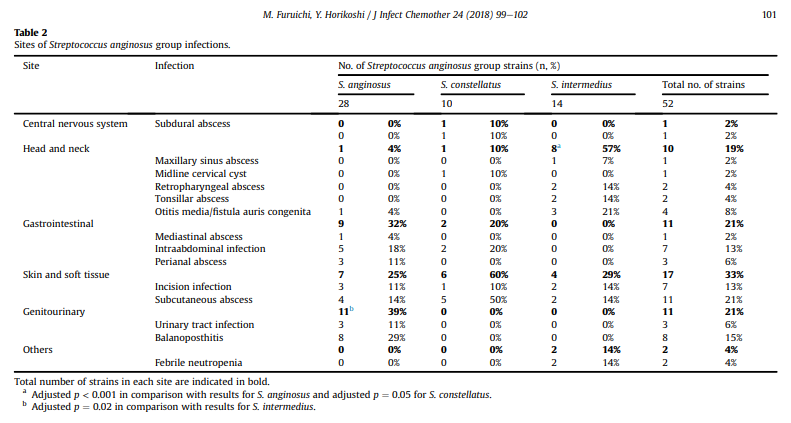
Pediatric pts, Tokyo➡️87% polymicrobial; >70% of anginosus/constellatus with anaerobes (esp Bacteroides)
👉pubmed.ncbi.nlm.nih.gov/28918832/
Adult pts, NY➡️70% polymicrobial; GN anaerobes, enterobacteriaceae common
~¾ S.anginosus infections = polymicrobial
👉pubmed.ncbi.nlm.nih.gov/29050796/
Pediatric pts, Tokyo➡️87% polymicrobial; >70% of anginosus/constellatus with anaerobes (esp Bacteroides)
👉pubmed.ncbi.nlm.nih.gov/28918832/
Adult pts, NY➡️70% polymicrobial; GN anaerobes, enterobacteriaceae common
7/
⚡️S.anginosus bacteremia should prompt investigation for underlying suppurative infection (can be occult)⚡️
🔸Normal flora oral cavity, H&N, GI tract
🔸Can enter circulation w/o obvious site of trauma or infection
🔸Range fr relatively minor oral infection to severe abscess
⚡️S.anginosus bacteremia should prompt investigation for underlying suppurative infection (can be occult)⚡️
🔸Normal flora oral cavity, H&N, GI tract
🔸Can enter circulation w/o obvious site of trauma or infection
🔸Range fr relatively minor oral infection to severe abscess
8/
🗣️H&N infections can spread to deep spaces via local extension
🗣️Possible complications: airway obstruction, jugular V septic thrombophlebitis (Lemierres), peritonsillar abscess, cervical nec fasc, orbital cellulitis
🧠Can lead to brain abscess
🗣️H&N infections can spread to deep spaces via local extension
🗣️Possible complications: airway obstruction, jugular V septic thrombophlebitis (Lemierres), peritonsillar abscess, cervical nec fasc, orbital cellulitis
🧠Can lead to brain abscess
9/
⭐️Consider intra-abdominal or liver abscess, cholangitis, peritonitis, abd wound inf
⭐️S.anginosus + acute appendectomy. Here is 1 ref: 26% intra-op cx +S.anginosus➡️ associated with complicated appy, longer LOS, ⬆️likelihood of post-op collection:
pubmed.ncbi.nlm.nih.gov/29241966/
⭐️Consider intra-abdominal or liver abscess, cholangitis, peritonitis, abd wound inf
⭐️S.anginosus + acute appendectomy. Here is 1 ref: 26% intra-op cx +S.anginosus➡️ associated with complicated appy, longer LOS, ⬆️likelihood of post-op collection:
pubmed.ncbi.nlm.nih.gov/29241966/
10/
🫁Would also mention pneumonia, lung abscess/empyema, and mediastinitis/abscess as well
🫀Rarely can cause endocarditis as well as SSTI, osteomyelitis, septic arthritis
🫁Would also mention pneumonia, lung abscess/empyema, and mediastinitis/abscess as well
🫀Rarely can cause endocarditis as well as SSTI, osteomyelitis, septic arthritis
11/
Tx:
🩹Source control, debrid/drainage PRN
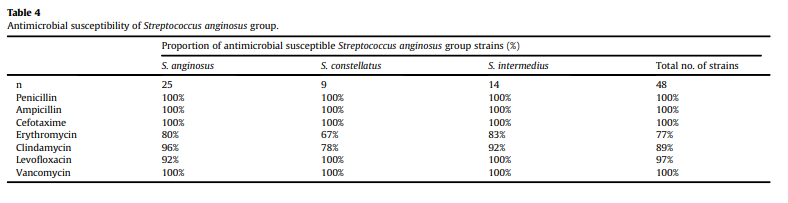
💊Ceftriaxone = preferred agent
💊Typically low PCN MICs but rarely can have PCN-intermediate or R strains with altered PBPs
💊Less ideal but possible alternatives: Vanc, FQ
💊Don't forget that some might need anaerobic tx
Tx:
🩹Source control, debrid/drainage PRN
💊Ceftriaxone = preferred agent
💊Typically low PCN MICs but rarely can have PCN-intermediate or R strains with altered PBPs
💊Less ideal but possible alternatives: Vanc, FQ
💊Don't forget that some might need anaerobic tx
• • •
Missing some Tweet in this thread? You can try to
force a refresh