
1) There is a lot of talk about decaying antibodies. I would like to walk you through a few findings about antibodies to SARS-CoV-2 that we put on medRxiv on Friday. Ill do this slowly over the day (while being in nonstop conference calls). But I feel this needs to get out there.
2) So, here is a link to that paper: medrxiv.org/content/10.110…. It is simple and pretty straight forward. Three figures only.
3) Before we start, two things: Acknowledgments and a primer in B-cell biology (a simple one):
4) Acknowledgements: This was spearheaded by Dr. Ania Wajnberg at Mount Sinai Hospital, Dr. Carlos Cordon-Cardo who runs the clinical lab at Sinai's Pathology Department and my team here at the Microbiology Department with @FatimaAmanat @Shirin_Strohm @DanielStadlb @Babagannoosh
5) Simple B-cell biology. B-cells make antibodies. Not all, all the time, but let me explain in a simple way. When you get infected, initial subsets of B-cells called plasmablasts get activated and make tons of antibody a few days after infection. They are responsible for your...
6)....initial antibodies. They die after about two weeks but their antibodies stay for some time since IgG antibodies have a half life of approximately 21 days. Of course the antibody levels from these initial plasmablasts will start to go down after some time. But......
7)...there is also a second set of B-cells that secrete antibodies and gets activated (complicated process). They migrate mostly to the bone marrow and just sit there and make antibodies, often for a long time (that's why they are called long-lived plasma cells).....
8) They are the ones that maintain your serum antibody levels for a long time, sometimes life long (probably shorter for coronaviruses). And then, there is a third set of B-cells. They are called memory B-cells. They actually don't make antibody. But they get quickly......
9)...reactivated and become plasmablasts if you get reinfected. This quick plasmablast response might prevent you from getting severe disease or even from getting symptoms after re-infection. So, to recap.....
10)...initially you get a lot of antibodies from plasmablast, these antibodies go down after weeks to months and then usually hit a stable titer which is maintained by the bone-marrow residing plasma cells. So, you expect a peak, a decline and a stabilization phase.
11) This sets the stage for the new preprint. First, Carlos' lab screened >50,000 people using an anti-spike ELISA that my lab designed. In their shop it is FDA emergency use authorized, by the way. These people were screened to look for potential convalescent plasma donors....
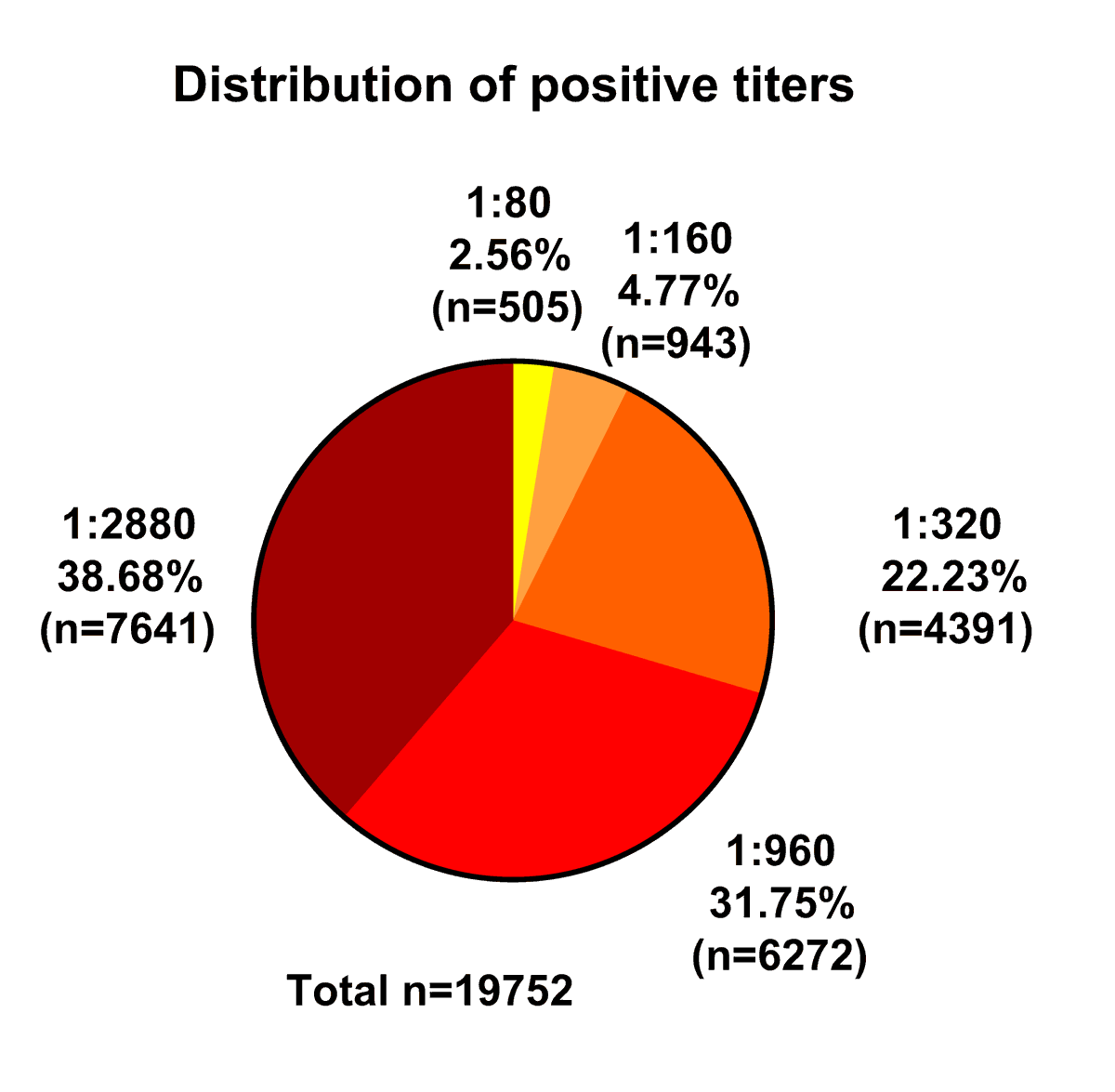
12)....or because they were employees that wanted to know if they seroconverted. Of the 50,000 people Carlos identified >19,000 people with antibodies to SARS-CoV-2. Those are mostly from mild or even asymptomatic cases.
13) Now, how did their antibody responses look like? Very few had what we call low titers (1:80-1:160). About 22% had moderate titers (1:320). The remaining >70% had high titers (1:960-1:2880)...... 
14) We know that people with lower titers often have titer increase over time. It seems that people with mild infections often respond slower than severe cases. Keep that in mind, we will get back to that.
15) Now, what are these antibodies doing? They bind to the spike and spike antibodies can potentially neutralize the virus. So, we tested a range of titers for neutralization of real SARS-CoV-2 in a microneutralization assay. First, ELISA titers and neutralization correlate well.
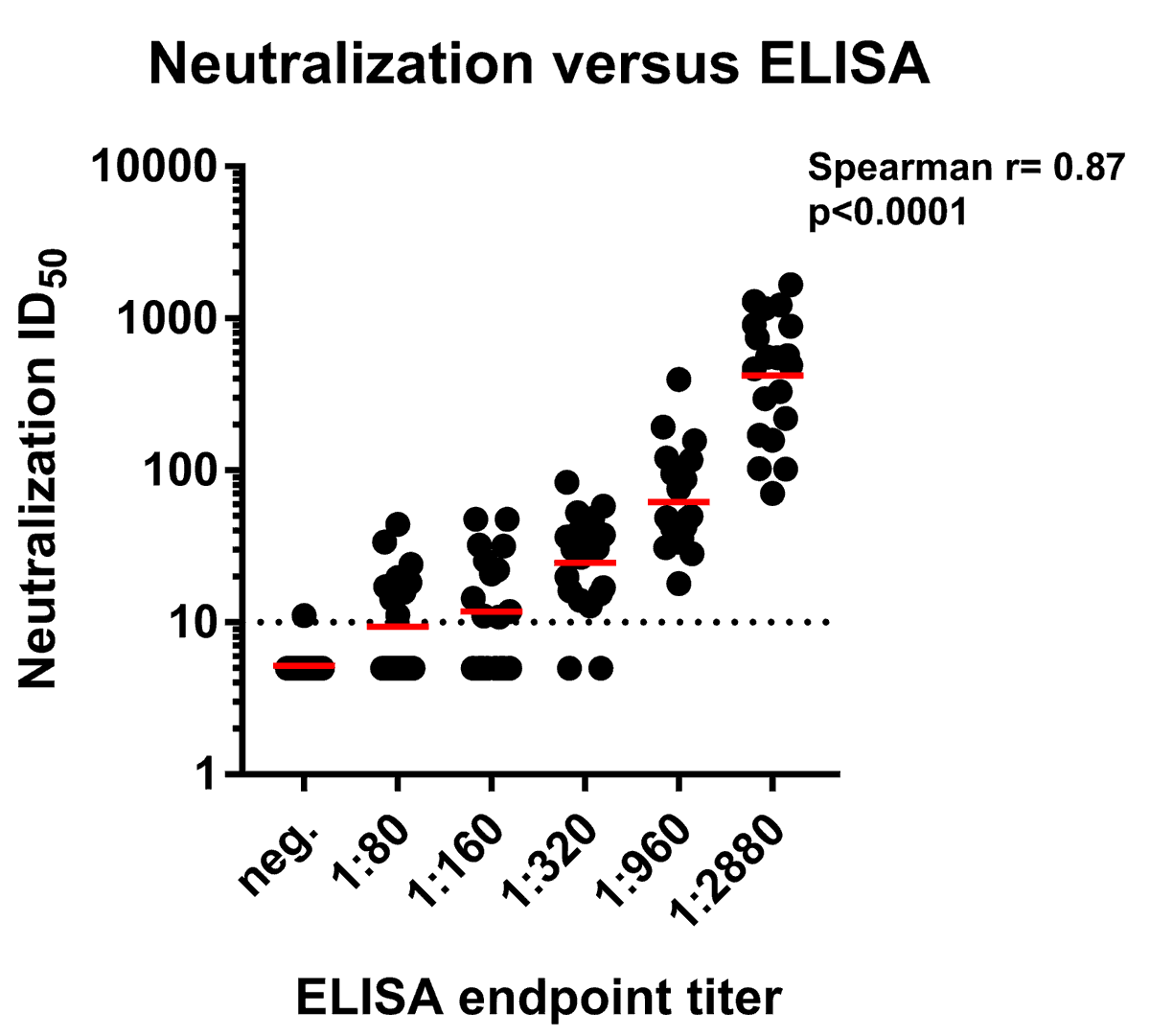
16) Of note, the variability in each titer category is high. But that is OK, since different people might target different epitopes, affinity maturation might be different etc.

17) Now, when looking at proportion of individuals who have any neutralizing activity, we see that about 50% of the 1:80-1:160 titers have neutralizing activity, 90% of the 1:320 titers have it and 100% of the titers above that have it.
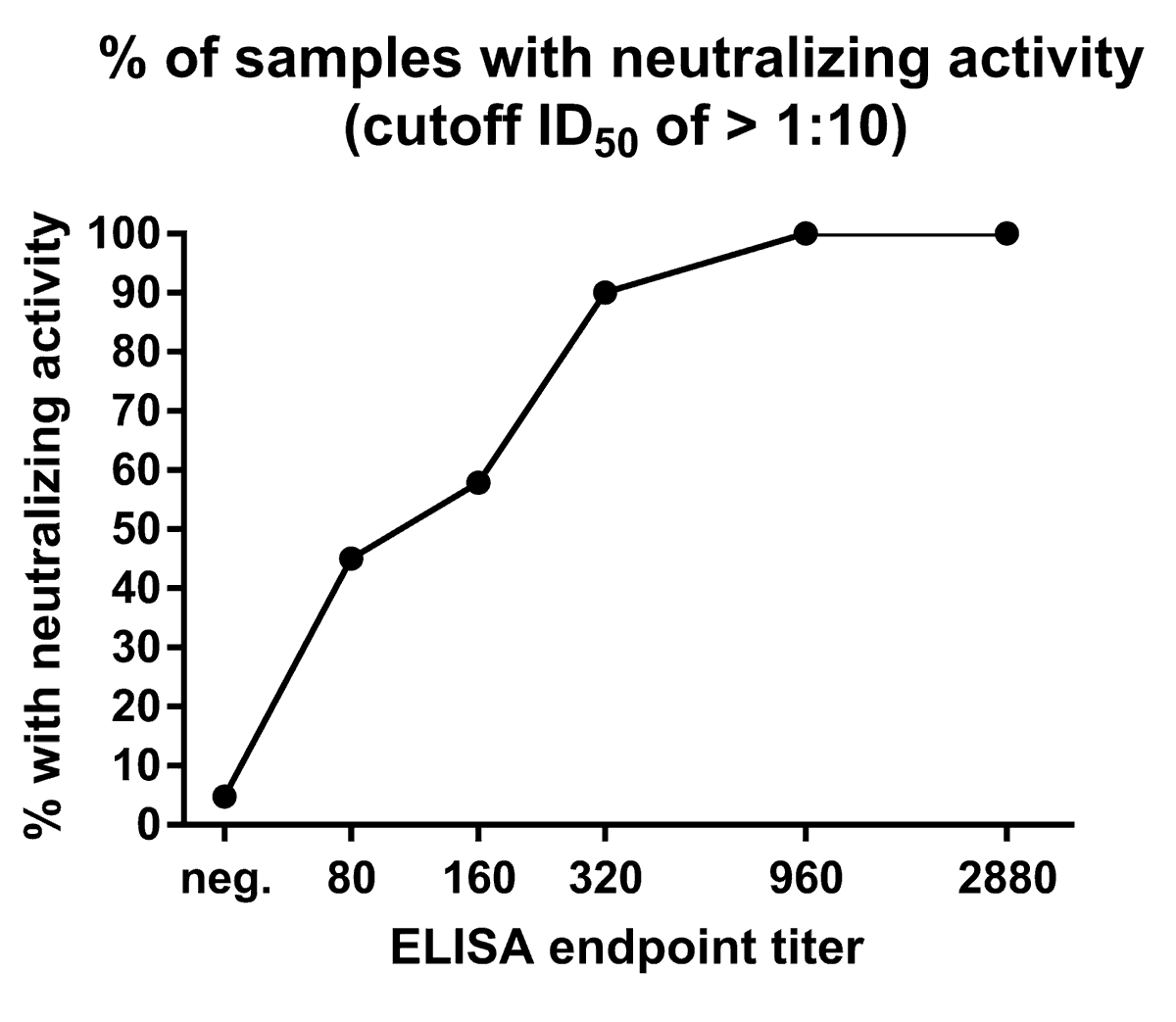
18) Of course, this is limited by the lower limit of detection of the neutralization assay (the assay is described in detail here if you are interested, open access of course: …rentprotocols.onlinelibrary.wiley.com/doi/full/10.10…).
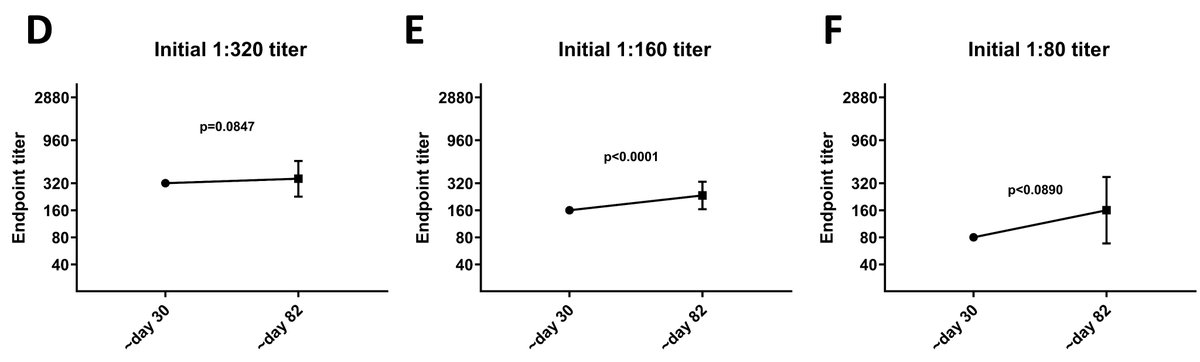
19) Now, how long lived are these antibodies (measured by ELISA against spike)? Dr. Wajnberg selected 121 individuals that were bled around 30 days after their initial symptom onset and brought them back at approximately 82 days after symptom onset.
20) But before telling you about the exciting data I have to jump on a conference call now😋 - stay tuned.
21) So, when we looked at the difference between day 30 and day 82 titers, we did see a decline. It was statistically significant but tiny.

22) To understand better what was going on, we started to stratify by initial titer. People who had high titers initially had - on average - decrease in titer. Not dramatic decreases (less than 3-fold) but certainly appreciable.
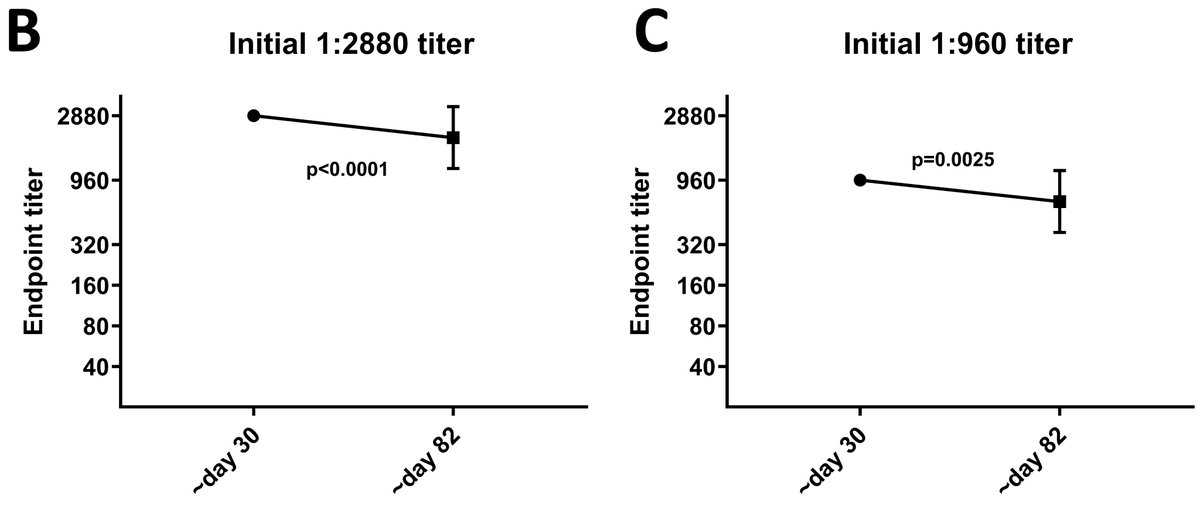
23) People with moderate to low titers however, hat increases. Again, they were not huge but for sure there was an upwards trend. As mentioned earlier, mild cases often need time until their antibody titers go up.
24) So, first, a few caveats: We did not measure the neutralizing titers at the later time point. While we assume the neutralization titers stay the same, we haven't proven that yet. Ratios of neutralizing versus non-neutralizing antibodies might change over time.
25) Another caveat is the low number of samples for the neutralization and longitudinal analysis. Also, we had mostly mild cases, disease severity might influence this. Also the highest titer the assay in the clinical lab measures is >1:2880, everything above is also registered..
26)...as >2880, so we are missing some resolution there.....
27) Now, how does this compare to data from other labs? I think the actual data compares pretty well. There are a lot of 'oh my god the antibodies are going down' headlines, but a lot of data suggests a slow and expected decline over months - which I think is normal.
28) Here are the important questions (which we can't answer yet): What is the long-term baseline titer going to be? How long-lived will that be? How much antibody will you need to be protected from reinfection? How much antibody do you need to be protected from disease?
29) These are important questions and we need to answer them with appropriate studies. Importantly, specific antibody titers that indicate protection (correlates of protection) have been established for influenza, measles, hepatitis A, hepatitis B etc.
30) We need to define this titer for SARS-CoV-2 as well. A combination of a protective titers plus detailed knowledge of specific antibody kinetic would allow us to make predictions who is at risk and who is not. This is also important for vaccine development and...
31) ...development of vaccination regimens (e.g. to determine when you need a booster dose). The important part to keep in mind is, that even if we define a protective titer, this titer will be associated with a reduction in risk. That doesn't not mean that re-infections.....
32)....are impossible. Just not likely. Keep that in mind too. In the end it all boils down to probabilities.
33) PS: I did not mention T-cells. But I will get back to that in another Tweetorial.

