
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 25y/oM quit🚬3 mos ago, now 3🩸loose BM/day,mild abdo cramps;Cousin w Crohns;Stool➖for infection;CLN: erythematous granular mucosa rectum+sigmoid, superficial ulcers;BX:Acute cryptitis,crypt abscess,crypt architecture distortion. What helps most dx UC vs Crohn’s?
#B2B #IBDPoll
#B2B #IBDPoll
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty UC and CD:
🔻Chronic inflammation of the GI tract
🔻Affects all ages: Typically starts between age 20-39
🔻Second peak of incidence age >50
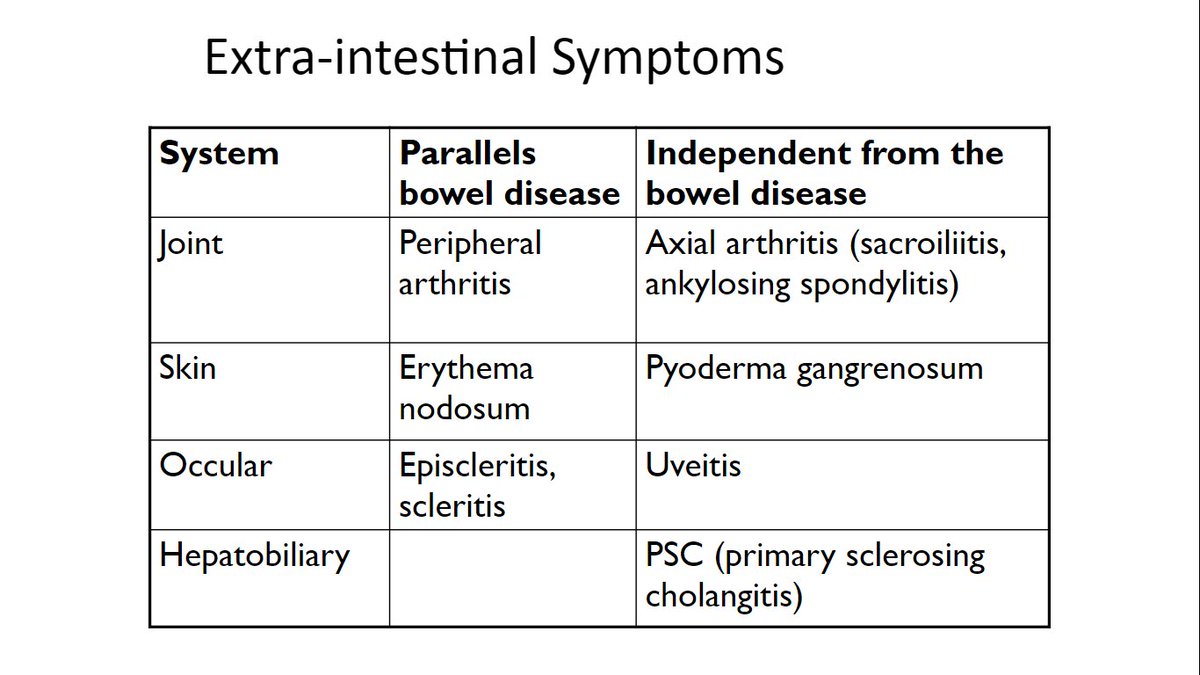
🔻Flares of GI symptoms +/-systemic symptoms +/- EIM
🔻Chronic inflammation of the GI tract
🔻Affects all ages: Typically starts between age 20-39
🔻Second peak of incidence age >50
🔻Flares of GI symptoms +/-systemic symptoms +/- EIM
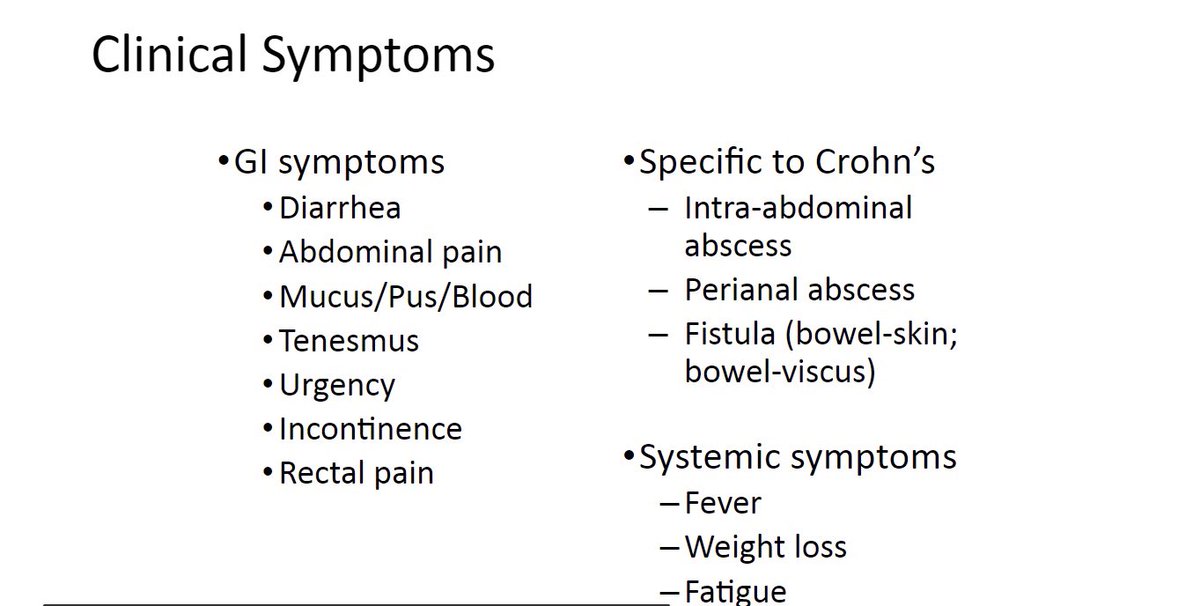
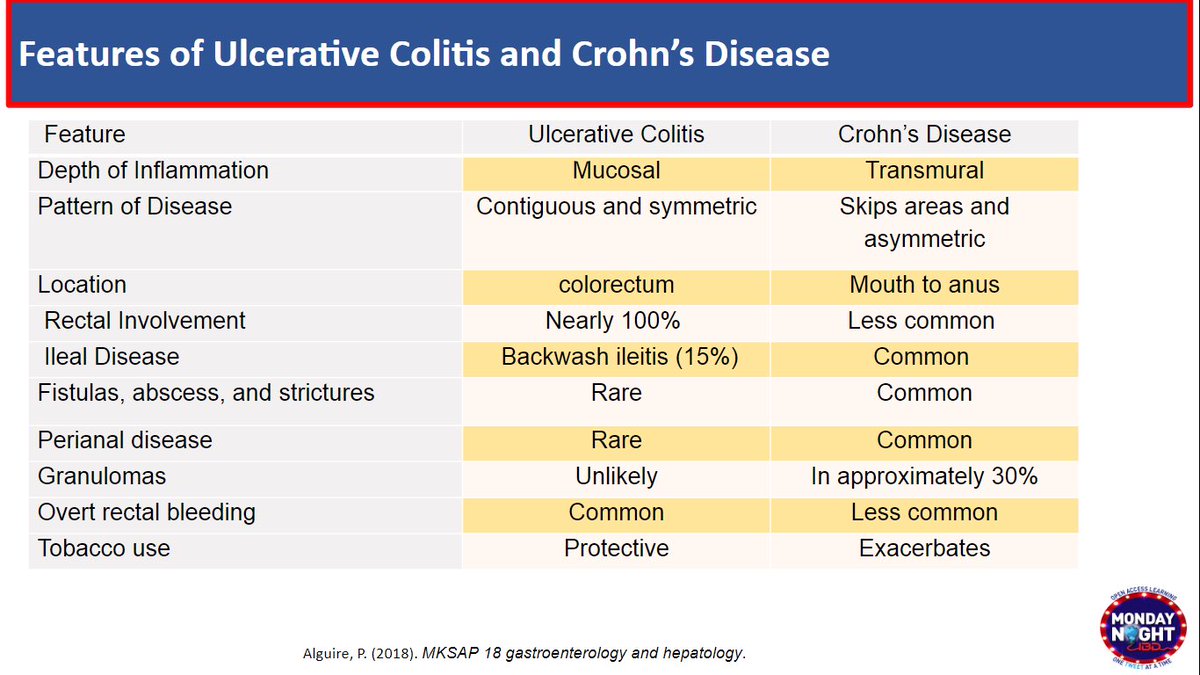
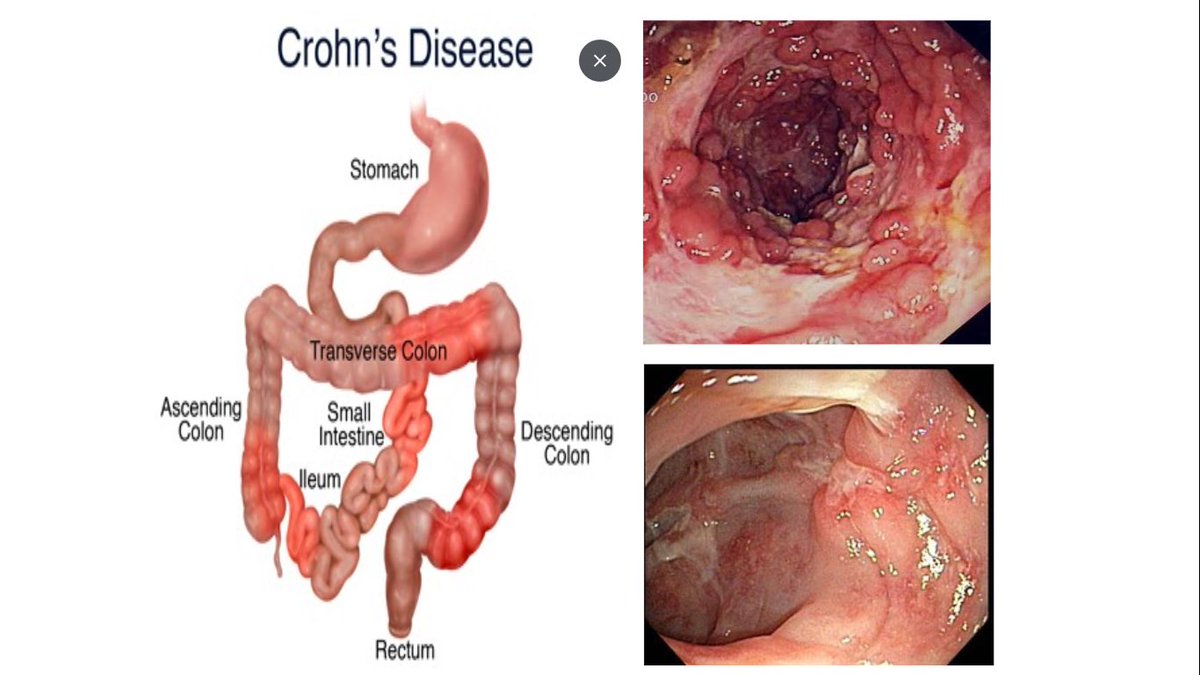
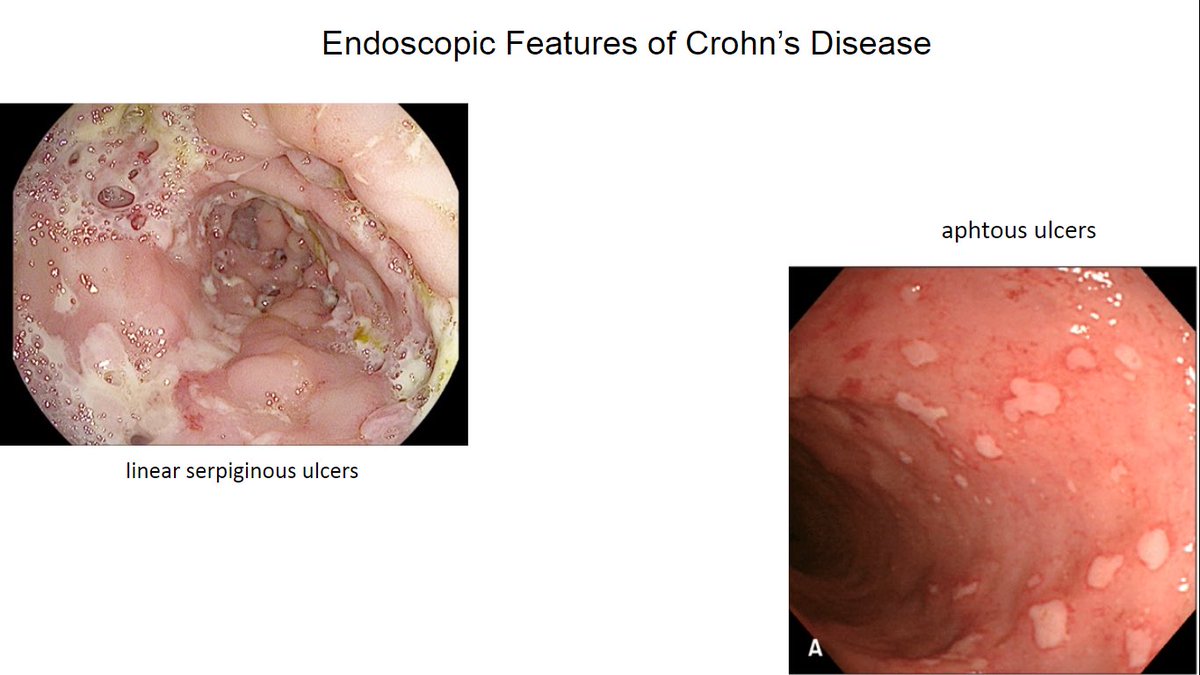
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 3/ CD:
💡Skipped lesion, any part of GI tract
💡Most common:Colon+ileum
Hallmark➡️ulcers: aphthous,deep large/linear/serpiginous
💡Transmural inflamm -> stricturing, perforating dis.
🚩#B2BPearl
👉🏼Rectum can be involved in CD;➕anorectal ulcers → ⬆️risk of perianal disease
💡Skipped lesion, any part of GI tract
💡Most common:Colon+ileum
Hallmark➡️ulcers: aphthous,deep large/linear/serpiginous
💡Transmural inflamm -> stricturing, perforating dis.
🚩#B2BPearl
👉🏼Rectum can be involved in CD;➕anorectal ulcers → ⬆️risk of perianal disease
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 4/ Ulcerative Colitis:
📍Hallmark symptoms: rectal bleeding
📍Typically in ex-smoker 🚬
📍Superficial Inflammation limited to mucosa and submucosa.
📍Endoscopy:
Rectum (almost👇🏼) always involved
📍Can extend proximally from rectum in a continuous fashion
📍Hallmark symptoms: rectal bleeding
📍Typically in ex-smoker 🚬
📍Superficial Inflammation limited to mucosa and submucosa.
📍Endoscopy:
Rectum (almost👇🏼) always involved
📍Can extend proximally from rectum in a continuous fashion
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 5/ UC in endo
🚩#B2BPearls:
📌UC+PSC -> Rectal sparing
📌Cecal patch = periappendiceal inflammation w proctitis/ Left-sided colitis ≠Crohns’ skipped lesions
📌Backwash ileitis with severe pancolitis ≠Crohns ileocolitis
🚩#B2BPearls:
📌UC+PSC -> Rectal sparing
📌Cecal patch = periappendiceal inflammation w proctitis/ Left-sided colitis ≠Crohns’ skipped lesions
📌Backwash ileitis with severe pancolitis ≠Crohns ileocolitis
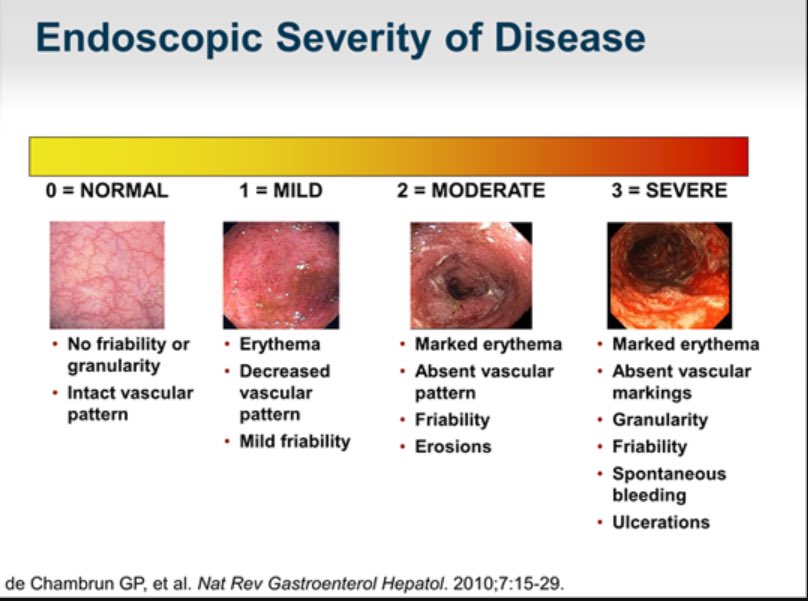
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 6/ UC Mayo:
🔎 Mayo 1: erythema,⬇️ vascular pattern,mild friability
🔎 Mayo 2:marked erythema, absent vascular pattern, friability, erosions
🔎 Mayo 3: deep ulcerations+ spontaneous 🩸
💎 #B2BPearl: Clinical Sx don’t always↔️endo activity
✅ CRP, FCP 👉🏼monitor dz+Rx response
🔎 Mayo 1: erythema,⬇️ vascular pattern,mild friability
🔎 Mayo 2:marked erythema, absent vascular pattern, friability, erosions
🔎 Mayo 3: deep ulcerations+ spontaneous 🩸
💎 #B2BPearl: Clinical Sx don’t always↔️endo activity
✅ CRP, FCP 👉🏼monitor dz+Rx response
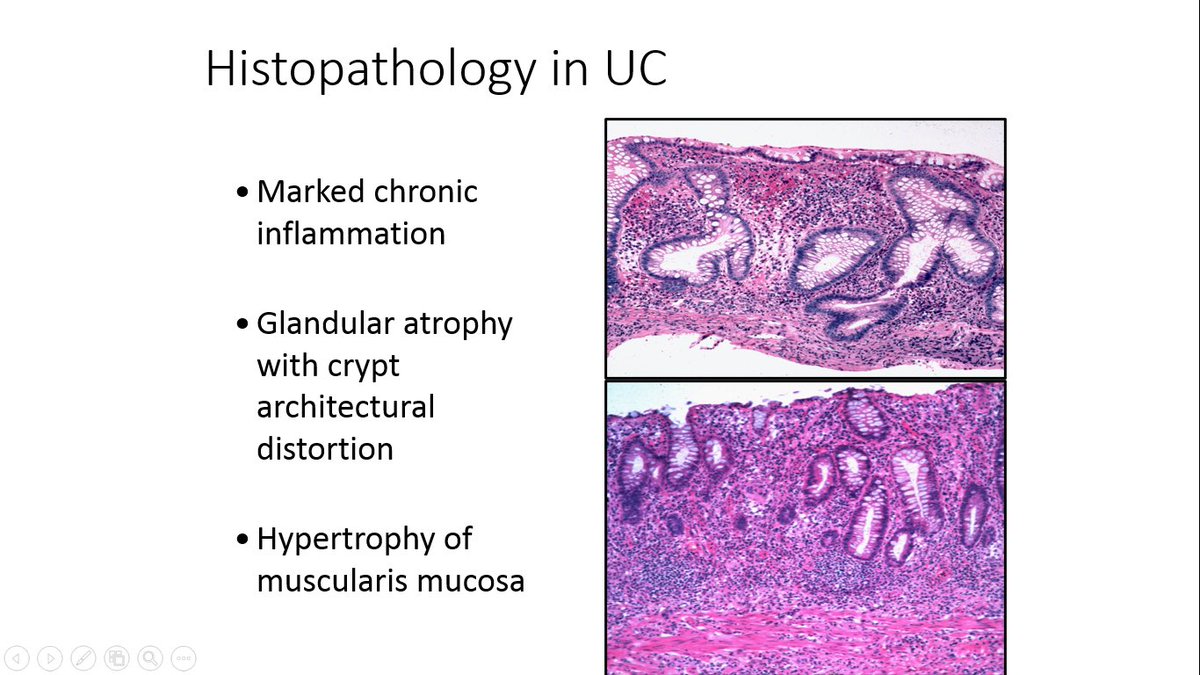
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 7/ What about #GIPath ❓
🚩Acute colitis features: acute cryptitis, crypt abscess
📍Present in any acute inflammation: infection, drug reaction, IBD
🚩Look for additional signs of chronicity to make Dx of IBD
📍Crypt architecture distortion, depletion of goblet cells
🚩Acute colitis features: acute cryptitis, crypt abscess
📍Present in any acute inflammation: infection, drug reaction, IBD
🚩Look for additional signs of chronicity to make Dx of IBD
📍Crypt architecture distortion, depletion of goblet cells
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 8/
✨ #GIPath #B2BPearl
Path alone can not ≠ UC vs CD
Except if + non-caseating epithelioid granuloma: + <30% of CD
✨ #B2BPearl
Crypt-associated granulomas can be seen in UC !
@UmaMahadevanMD 10.1046/j.1365-2559.2002.01416.x
✨ #GIPath #B2BPearl
Path alone can not ≠ UC vs CD
Except if + non-caseating epithelioid granuloma: + <30% of CD
✨ #B2BPearl
Crypt-associated granulomas can be seen in UC !
@UmaMahadevanMD 10.1046/j.1365-2559.2002.01416.x
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty 9/ What about IBD serologies?
🔺Autoantibodies & Antibodies to microbial antigens:
⬆️ assoc pANCA & UC
⬆️ assoc of ASCA, OmpC, anti-I2, anti-Flagellin & CD
🔺But NOT sensitive or specific
✨#B2BPearl:🚫Routine use of IBD serologies for Dx/differentiate UC & CD @AmCollegeGastro
🔺Autoantibodies & Antibodies to microbial antigens:
⬆️ assoc pANCA & UC
⬆️ assoc of ASCA, OmpC, anti-I2, anti-Flagellin & CD
🔺But NOT sensitive or specific
✨#B2BPearl:🚫Routine use of IBD serologies for Dx/differentiate UC & CD @AmCollegeGastro
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 10/ Rx choice depends on extent AND severity of UC:
Today🔍on 5-ASA for mild-moderate UC
👉🏼PR >PO for proctitis Sx (urgency, tenesmus, rectal bleeding)
PR Supp->rectum
PR Enema->sigmoid
✨#B2BPearl: Give PR at bedtime!
👉🏼Combo PO+PR> PO alone
🔹 Mild-Mod UC: 2.4g- 4.8g/day
Today🔍on 5-ASA for mild-moderate UC
👉🏼PR >PO for proctitis Sx (urgency, tenesmus, rectal bleeding)
PR Supp->rectum
PR Enema->sigmoid
✨#B2BPearl: Give PR at bedtime!
👉🏼Combo PO+PR> PO alone
🔹 Mild-Mod UC: 2.4g- 4.8g/day
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 11/How do 5-ASA work?
🔻5-ASA released in the bowel & act like a topical agent to the mucosa
🔻20% of the 5ASA get absorbed
Excreted by kidney
🔻For induction + maintenance
🏁As a general rule keep same dose that induced remission for maintenance
🔻5-ASA released in the bowel & act like a topical agent to the mucosa
🔻20% of the 5ASA get absorbed
Excreted by kidney
🔻For induction + maintenance
🏁As a general rule keep same dose that induced remission for maintenance
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 12/
Sulfasalazine (5-ASA +sulfapyridine):
👉🏼Oral
👉🏼Cheap
👉🏼Supplement w folic acid (‼️in pregnant women use FA 2m/gday)
👉🏼Reversible ⇩ sperm count/motility → stop if man trying to conceive
👉🏼High dose poorly tolerated: start low
👉🏼Contraindicated in Sulfa allergy
Sulfasalazine (5-ASA +sulfapyridine):
👉🏼Oral
👉🏼Cheap
👉🏼Supplement w folic acid (‼️in pregnant women use FA 2m/gday)
👉🏼Reversible ⇩ sperm count/motility → stop if man trying to conceive
👉🏼High dose poorly tolerated: start low
👉🏼Contraindicated in Sulfa allergy
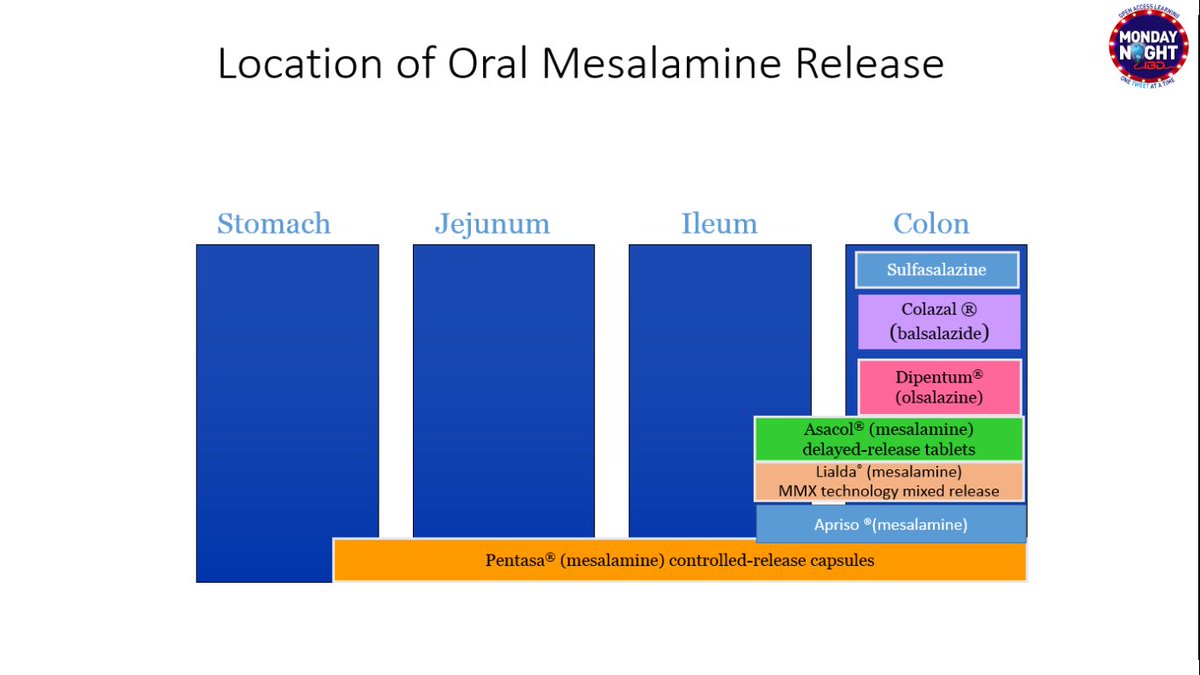
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 13/ Newer 5-ASA without Sulfa (mesalamine, olsalazine, balsalazide)
✔️Well tolerated
✔️Oral or topical
✔️Induction + maintenance
✔️Big several pills to take -> affect compliance
✔️Well tolerated
✔️Oral or topical
✔️Induction + maintenance
✔️Big several pills to take -> affect compliance
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 14/ 5-ASA are safe but have SEs
✨#B2BPearl: Can ⇧ diarrhea in 2-3% population
🚨Interstitial Nephritis (elderly, comorbidities)
🚨Pancreatitis
🚨Pericarditis & Pleuritis
🚨Pneumonitis
‼️Alert pt of symptoms to watch for‼️
✨#B2BPearl: Can ⇧ diarrhea in 2-3% population
🚨Interstitial Nephritis (elderly, comorbidities)
🚨Pancreatitis
🚨Pericarditis & Pleuritis
🚨Pneumonitis
‼️Alert pt of symptoms to watch for‼️
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro 15/So to recap
⛱ UC &CD Dx based on combo clinical+endo findings
⛱ Bx:✅chronic+acute changes of colitis
⛱ Path alone can not ≠ UC vs CD
Except if +epithelioid granulomas of CD
⛱ 1st line Rx for Mild UC: 5ASA PO/PR
⛱ Overall safe but be aware of potential serious SEs
⛱ UC &CD Dx based on combo clinical+endo findings
⛱ Bx:✅chronic+acute changes of colitis
⛱ Path alone can not ≠ UC vs CD
Except if +epithelioid granulomas of CD
⛱ 1st line Rx for Mild UC: 5ASA PO/PR
⛱ Overall safe but be aware of potential serious SEs
@MondayNightIBD @SobiaMujtabaMD @DuekerJeffrey @DCharabaty @AmCollegeGastro @SobiaMujtabaMD @Waseem_AhmedMD @JeanDonet @LizzieAbyMD @DrMohdZein @AsadurRahman87 @DrMalSimons @Erica_Turse_DO @AdvaniRashmiMD @francisdaileymd @YIchkhanian @RomyChamoun @joshsteinbergMD @KM_Pawlak @GuiRamosMD @pricetedwards @HassaanZiaMD @SunnyOhSon @Marcfenster1

