Very excited to share our new preprint "#SARSCoV2 viral load dynamics, duration of viral shedding and infectiousness: a living systematic review and meta-analysis" #IDTwitter
A huge team effort screening and synthesising the accumulating evidence. 1/6
medrxiv.org/content/10.110…
A huge team effort screening and synthesising the accumulating evidence. 1/6
medrxiv.org/content/10.110…
2/6 Main findings:
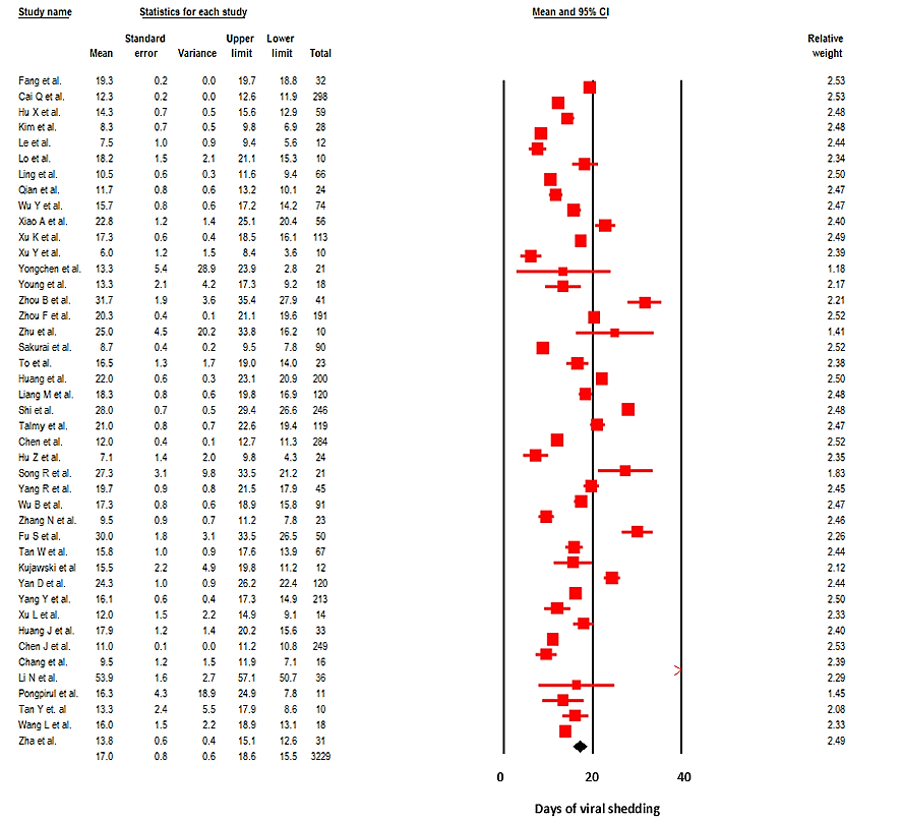
- In the upper respiratory tract (URT), mean duration of RNA shedding was 17 days (95% CI, 15.5-18.6), max 83d
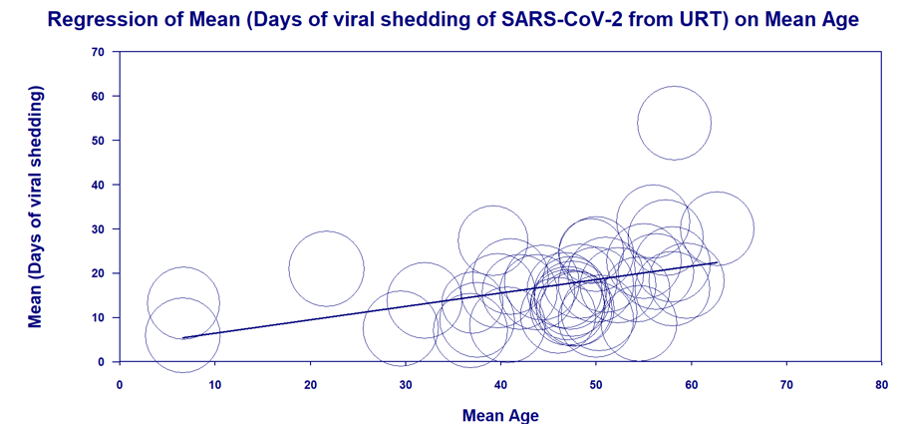
- Shedding duration increases with age & severity of illness
- There were limited studies reporting shedding duration in sputum (n=7) and stool (n=13)
- In the upper respiratory tract (URT), mean duration of RNA shedding was 17 days (95% CI, 15.5-18.6), max 83d
- Shedding duration increases with age & severity of illness
- There were limited studies reporting shedding duration in sputum (n=7) and stool (n=13)
3/6 - High SARS-CoV-2 viral loads in URT are detectable in the first week, and peak viral load occurs at day 0-5
- In contrast, peaks in SARS-1 and MERS occurred at days 10-14 and 7-10 of illness
- Pts with SARS-CoV-2 are likely to be most infectious day 0-5 (3/6)
- In contrast, peaks in SARS-1 and MERS occurred at days 10-14 and 7-10 of illness
- Pts with SARS-CoV-2 are likely to be most infectious day 0-5 (3/6)
4/6 - No study to date has cultured live virus beyond d9 in URT despite high viral loads (VL)
- The success of isolation correlated with VL quantified by PCR
- No successful viral culture when VL< 10^6 copies/ml, Ct values >24 or >34
- Only 2 studies cultured live virus in stool
- The success of isolation correlated with VL quantified by PCR
- No successful viral culture when VL< 10^6 copies/ml, Ct values >24 or >34
- Only 2 studies cultured live virus in stool
5/6 - Viral loads at the start of infection appear to be comparable in asymptomatic and symptomatic patients but most studies demonstrate faster viral clearance in asymptomatic individuals
- There are limited data on the shedding of infectious virus in asymptomatic individuals
- There are limited data on the shedding of infectious virus in asymptomatic individuals
6/6 This paper is now published in the @LancetMicrobe
It is a collaborative work of researchers from the @univofstandrews @Infection_StAnd ; Western General Hospital @ridu_nhsl , Edinburgh; Queen Elizabeth Hospital Glasgow; Cotugno Hospital, Naples & @CVRinfo @UofGlasgow
It is a collaborative work of researchers from the @univofstandrews @Infection_StAnd ; Western General Hospital @ridu_nhsl , Edinburgh; Queen Elizabeth Hospital Glasgow; Cotugno Hospital, Naples & @CVRinfo @UofGlasgow
https://twitter.com/mugecevik/status/1329817587367161857
• • •
Missing some Tweet in this thread? You can try to
force a refresh