1/
50M comes to clinic with severe pain on his index finger. It progressed to violaceous lesion with raised borders. PIP/DIP/MCP jts without effusion. No fevers and otherwise feels well.
Works as fisherman on the Cape
What organism?
#IDTwitter #MedTwitter #IDMedEd #FOAMed
50M comes to clinic with severe pain on his index finger. It progressed to violaceous lesion with raised borders. PIP/DIP/MCP jts without effusion. No fevers and otherwise feels well.
Works as fisherman on the Cape
What organism?
#IDTwitter #MedTwitter #IDMedEd #FOAMed
2/
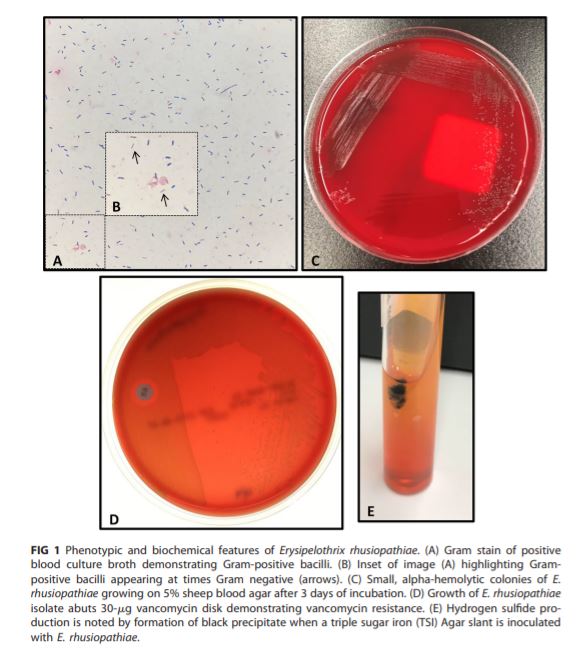
👍Correct answer = E.rhusiopathiae, a GP bacillus
🌳Widespread in nature, infecting domestic and marine animals
🦀Infections in humans often from occupational exposure: animal processing, butchers, fisherman, farmers, vets
🔽Break down clinical syndromes into 3 categories:
👍Correct answer = E.rhusiopathiae, a GP bacillus
🌳Widespread in nature, infecting domestic and marine animals
🦀Infections in humans often from occupational exposure: animal processing, butchers, fisherman, farmers, vets
🔽Break down clinical syndromes into 3 categories:
3/
1) Localized cutaneous (erysipeloid) inf, most common
▪️Subacute cellulitis, often hands/fingers (site of exposure), abrasion/wound can be portal of entry
▪️Might hear: seafood packer handling contaminated 🐟/🦀or similar -- but also think about w/😼🐶bites
▪️Incubation: 2-7d
1) Localized cutaneous (erysipeloid) inf, most common
▪️Subacute cellulitis, often hands/fingers (site of exposure), abrasion/wound can be portal of entry
▪️Might hear: seafood packer handling contaminated 🐟/🦀or similar -- but also think about w/😼🐶bites
▪️Incubation: 2-7d
4/
▪️pain at site➡️red macule➡️violaceous lesion: central clearing, raised border
▪️minimal swelling
▪️ 🚫systemic sxs
▪️Local lymphangitis/adenitis ~1/3 cases
2) Diffuse cutaneous
▪️Progress fr inoculation site +/- addl sites
▪️Can appear urticarial, bullous
▪️Can have fever
▪️pain at site➡️red macule➡️violaceous lesion: central clearing, raised border
▪️minimal swelling
▪️ 🚫systemic sxs
▪️Local lymphangitis/adenitis ~1/3 cases
2) Diffuse cutaneous
▪️Progress fr inoculation site +/- addl sites
▪️Can appear urticarial, bullous
▪️Can have fever



5/
3) Systemic, rare
🌡️Fever, sepsis
▪️40% antecedent or concurrent lesions
▪️Serpiginous lesions or mult bullous lesion on trunk/ext
⭐️Chronic liver dz, ICH ⬆️ risk
🫀Can see endocarditis. Esp, native AoV. Often extensive destruction
▪️Other rare cxs reported (PJI, abscess, etc)
3) Systemic, rare
🌡️Fever, sepsis
▪️40% antecedent or concurrent lesions
▪️Serpiginous lesions or mult bullous lesion on trunk/ext
⭐️Chronic liver dz, ICH ⬆️ risk
🫀Can see endocarditis. Esp, native AoV. Often extensive destruction
▪️Other rare cxs reported (PJI, abscess, etc)
6/
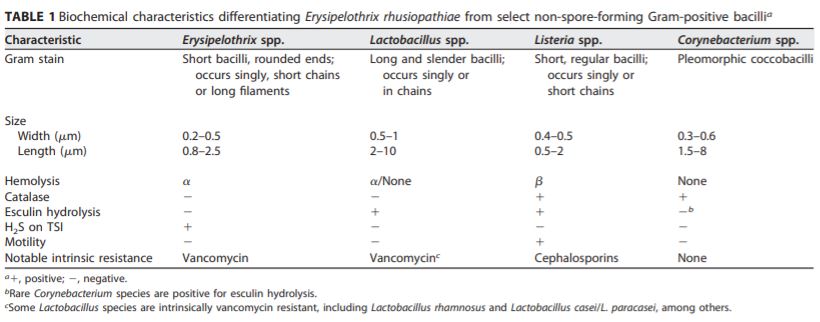
Dx: grows on routine cx but can be misidentified. GS, colony morphology, neg catalase might confuse w/Lactobacillus, Actinomyces, Arcanobact, Strep, or Enterococcus
ncbi.nlm.nih.gov/pmc/articles/P…
jcm.asm.org/content/57/6/e…
Like always, clinical hx and context is key here.
Dx: grows on routine cx but can be misidentified. GS, colony morphology, neg catalase might confuse w/Lactobacillus, Actinomyces, Arcanobact, Strep, or Enterococcus
ncbi.nlm.nih.gov/pmc/articles/P…
jcm.asm.org/content/57/6/e…
Like always, clinical hx and context is key here.
7/
Reasons to favor dx of erysipeloid over other pathogens, in particular strep/staph cellulitis:
🧩Occup exposure
🧩Lesion on fingers
🧩Subacute course
🧩Violaceous appearance
🧩Pain out of proportion
🧩A cellulitis not responding to Vanc monotherapy
Reasons to favor dx of erysipeloid over other pathogens, in particular strep/staph cellulitis:
🧩Occup exposure
🧩Lesion on fingers
🧩Subacute course
🧩Violaceous appearance
🧩Pain out of proportion
🧩A cellulitis not responding to Vanc monotherapy
8/
Erysipeloid skin lesions can resolve w/o therapy in wks but abxs shorten illness,⬇️relapse risk
Abx options = PCN, amox, cephalosporins
Others: imipenem, FQ, clinda, dapto, lzd
🚨Remember intrinsic R to Vanc! Also usu R to TMP-SMX, AG. Tetracyclines not consistently active
Erysipeloid skin lesions can resolve w/o therapy in wks but abxs shorten illness,⬇️relapse risk
Abx options = PCN, amox, cephalosporins
Others: imipenem, FQ, clinda, dapto, lzd
🚨Remember intrinsic R to Vanc! Also usu R to TMP-SMX, AG. Tetracyclines not consistently active
9/
Trivia:
⭐️Prior names = Rosenbach's disease, swine erysipelas, rouget du porc (French), mal rossino (Italian)
⭐️1st isolated from mice by Robert Koch 1878, swine by Louis Pasteur 1882 --> ID'd as human pathogen in 1909 by Rosenbach, who coined erysipeloid
Trivia:
⭐️Prior names = Rosenbach's disease, swine erysipelas, rouget du porc (French), mal rossino (Italian)
⭐️1st isolated from mice by Robert Koch 1878, swine by Louis Pasteur 1882 --> ID'd as human pathogen in 1909 by Rosenbach, who coined erysipeloid
10/
Photo credits and ref:
pubmed.ncbi.nlm.nih.gov/19663854/
pubmed.ncbi.nlm.nih.gov/19486064/
atlasdermatologico.com.br/disease.jsf;js…
Mandell
Photo credits and ref:
pubmed.ncbi.nlm.nih.gov/19663854/
pubmed.ncbi.nlm.nih.gov/19486064/
atlasdermatologico.com.br/disease.jsf;js…
Mandell