1/
First #IDtweetorial
65M w/persistent MRSA bacteremia on day 4 of Vancomycin. Last Vanc trough 18.7. MRSA is Vanco Susc.
Primary team asking to change therapy.
What would you do? (Poll)
Let’s review some of the evidence to guide our decision
#IDTwitter #IDfellows
First #IDtweetorial
65M w/persistent MRSA bacteremia on day 4 of Vancomycin. Last Vanc trough 18.7. MRSA is Vanco Susc.
Primary team asking to change therapy.
What would you do? (Poll)
Let’s review some of the evidence to guide our decision
#IDTwitter #IDfellows
2/
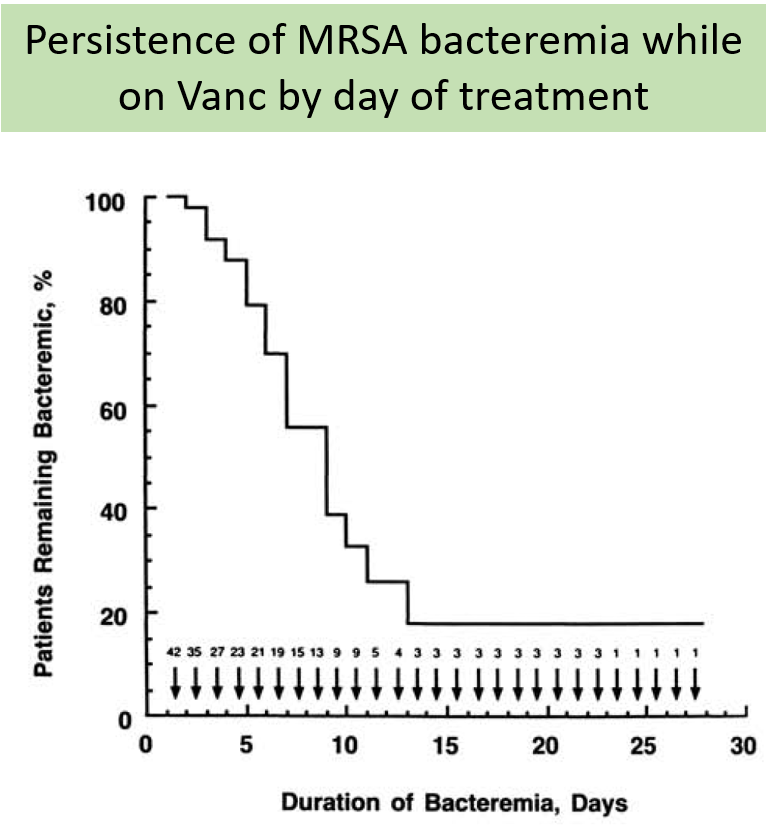
First, what is considered persistent bacteremia?
In a frequently cited study, bacteremia in pts w/MRSA IE lasted a median of 7d w/Vanco, w/ no unusual complications
This led to believe that slow clearance was usual for some cases of MRSA IE
bit.ly/2PDQ4wl
First, what is considered persistent bacteremia?
In a frequently cited study, bacteremia in pts w/MRSA IE lasted a median of 7d w/Vanco, w/ no unusual complications
This led to believe that slow clearance was usual for some cases of MRSA IE
bit.ly/2PDQ4wl
3/
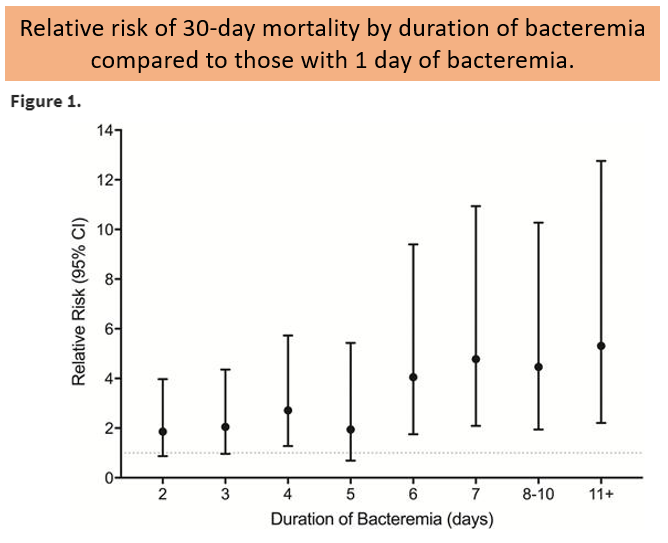
However, recent studies have shown significant increased risk in mortality and metastatic complications after 3 days of bacteremia.
bit.ly/31D7bnJ
However, recent studies have shown significant increased risk in mortality and metastatic complications after 3 days of bacteremia.
bit.ly/31D7bnJ
4/
So, our patient is at risk for complications (>3 days of bacteremia) and he is on adequate therapy. What can we do to help clear the blood cultures?
So, our patient is at risk for complications (>3 days of bacteremia) and he is on adequate therapy. What can we do to help clear the blood cultures?
5/
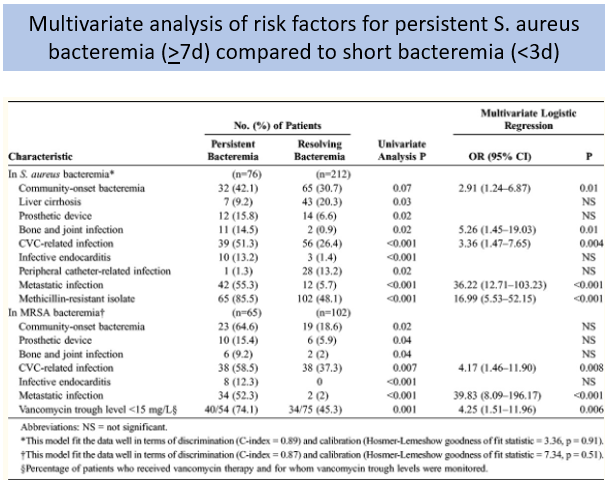
The answer is source control.
Persistent bacteremia has been associated with presence of hardware, metastatic infection, and endocarditis. All potentially removable foci of infection.
bit.ly/33D2jBE
The answer is source control.
Persistent bacteremia has been associated with presence of hardware, metastatic infection, and endocarditis. All potentially removable foci of infection.
bit.ly/33D2jBE
6/
Furthermore, in the previous study by Minejima et al., antibiotic therapy did not affect bacteremia duration, but longer time to source-control was associated with prolonged bacteremia.
bit.ly/31D7bnJ
Furthermore, in the previous study by Minejima et al., antibiotic therapy did not affect bacteremia duration, but longer time to source-control was associated with prolonged bacteremia.
bit.ly/31D7bnJ
7/
Source control is the most important thing. But let’s discuss if the antibiotic choice can help improve outcomes at all.
Source control is the most important thing. But let’s discuss if the antibiotic choice can help improve outcomes at all.
8/
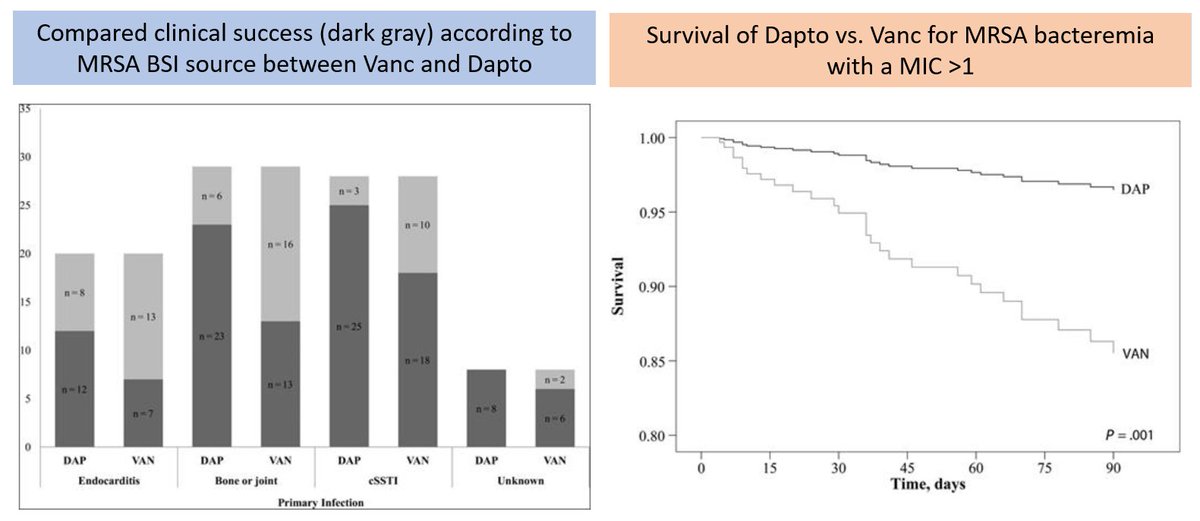
Some studies suggest better outcomes with Dapto compared to Vanco when MRSA has MIC > 1 to Vanco.
bit.ly/30K7EVG
A RCT to address this was stopped prematurely because of slow patient enrollment.
Our pt's MRSA has MIC < 1 for Vanco.
Some studies suggest better outcomes with Dapto compared to Vanco when MRSA has MIC > 1 to Vanco.
bit.ly/30K7EVG
A RCT to address this was stopped prematurely because of slow patient enrollment.
Our pt's MRSA has MIC < 1 for Vanco.
9/
CAMERA-2 trial compared adding an antistaphylococcal B-lactam (flucloxacillin, cloxacillin, or cefazolin) to Vanco or Dapto at start of therapy but did not show any benefits and was stopped because of AKI in the combination group. ja.ma/30tkmbm
CAMERA-2 trial compared adding an antistaphylococcal B-lactam (flucloxacillin, cloxacillin, or cefazolin) to Vanco or Dapto at start of therapy but did not show any benefits and was stopped because of AKI in the combination group. ja.ma/30tkmbm
10/
A RCT comparing standard therapy vs. Dapto+Ceftaroline combo as initial therapy was stopped early after 40 pts enrolled. Designed to assess duration of bacteremia, it had significant difference in in-hospital mortality (0% combo vs. 26% monotherapy)
bit.ly/33GuzTN
A RCT comparing standard therapy vs. Dapto+Ceftaroline combo as initial therapy was stopped early after 40 pts enrolled. Designed to assess duration of bacteremia, it had significant difference in in-hospital mortality (0% combo vs. 26% monotherapy)
bit.ly/33GuzTN
11/
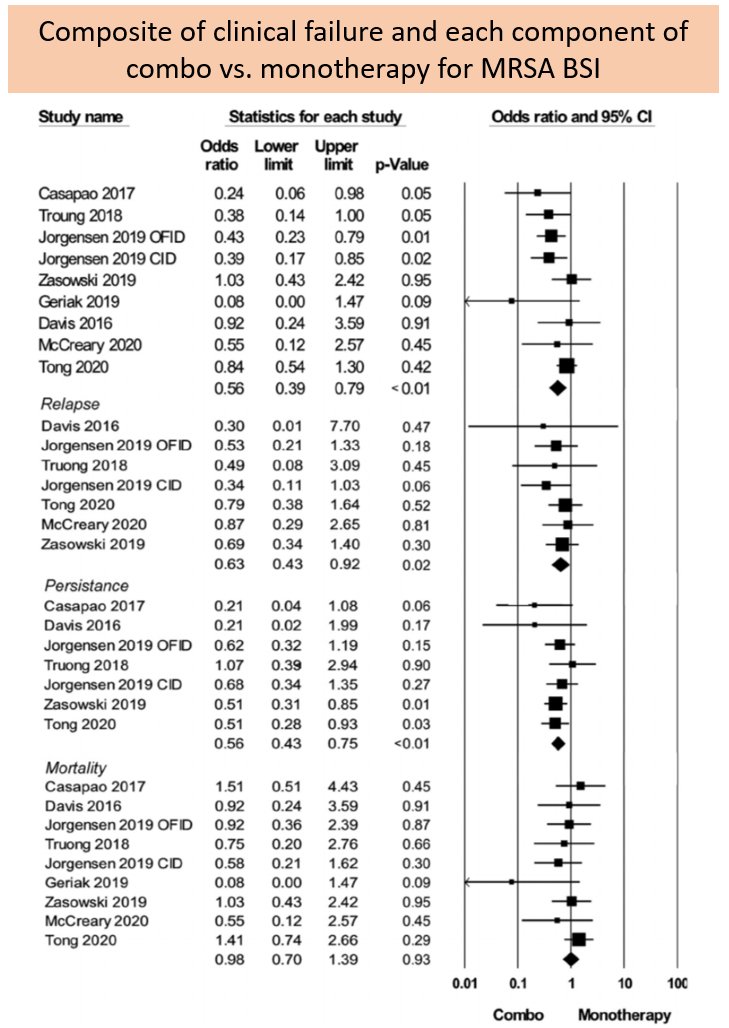
A recent meta-analysis (n=9; 3 RCT) of Dapto or Vanco against combo Vanco or Dapto + anti-MRSA B-lactam showed combo was associated w/ lower clinical failure rates, mainly driven by difference of bacteremia relapse and persistence, but no mortality.
bit.ly/3acEYaY
A recent meta-analysis (n=9; 3 RCT) of Dapto or Vanco against combo Vanco or Dapto + anti-MRSA B-lactam showed combo was associated w/ lower clinical failure rates, mainly driven by difference of bacteremia relapse and persistence, but no mortality.
bit.ly/3acEYaY
12/
Therefore combination therapy, specifically Dapto + Ceftaroline, the jury is still out. Combination may be considered in challenging cases as salvage therapy when source cannot be controlled.
Therefore combination therapy, specifically Dapto + Ceftaroline, the jury is still out. Combination may be considered in challenging cases as salvage therapy when source cannot be controlled.
13/
In summary,
1⃣Persistent bacteremia as short as 3 days⬆️risk of mortality & embolic events.
2⃣Source control, source control, source control. ASAP
3⃣Combo therapycan decrease duration of bacteremia but no clear evidence as of now of mortality benefit
Have a great monday!
In summary,
1⃣Persistent bacteremia as short as 3 days⬆️risk of mortality & embolic events.
2⃣Source control, source control, source control. ASAP
3⃣Combo therapycan decrease duration of bacteremia but no clear evidence as of now of mortality benefit
Have a great monday!