
1/
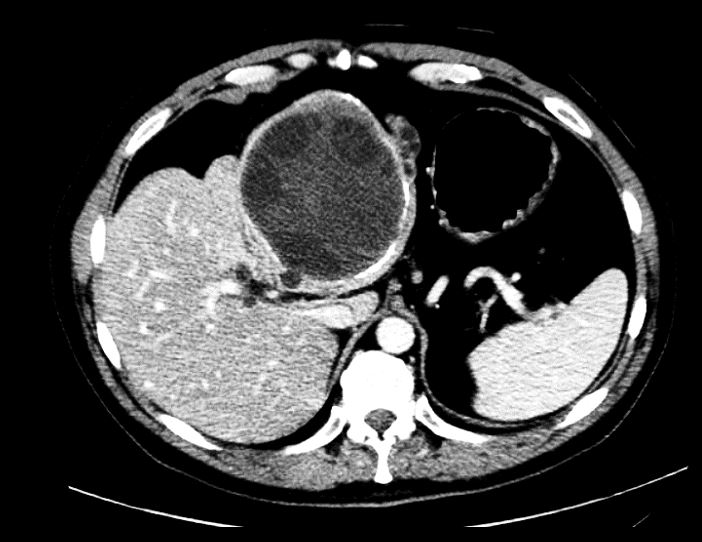
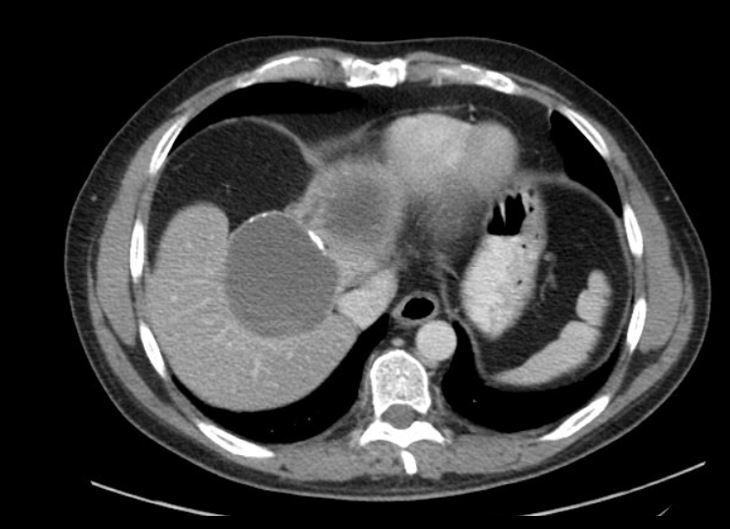
40M p/w abd pain off and on x 1 mo
No nausea, vomiting, diarrhea, fevers
Labs: WBC 14, T-bili 4.0, D-bili 2.8, ALT 220, AST 330, ALP 270
CT abd/pelvis imaging below
#IDTwitter #IDMedEd #IDFellows @ID_fellows
What is on your ddx?!
40M p/w abd pain off and on x 1 mo
No nausea, vomiting, diarrhea, fevers
Labs: WBC 14, T-bili 4.0, D-bili 2.8, ALT 220, AST 330, ALP 270
CT abd/pelvis imaging below
#IDTwitter #IDMedEd #IDFellows @ID_fellows
What is on your ddx?!
2/
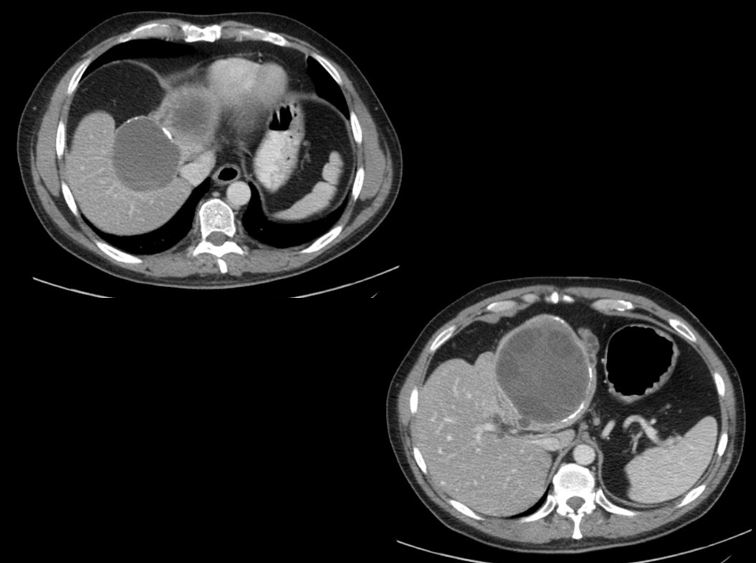
More images demonstrating multiple smaller cysts in the periphery of the dominant cyst
This distinct appearance gives the dx!
⭐️Cystic echinococcosis⭐️
More images demonstrating multiple smaller cysts in the periphery of the dominant cyst
This distinct appearance gives the dx!
⭐️Cystic echinococcosis⭐️


3/
🔹Dx was initially made radiographically ➡️ Started on albendazole
🔹Later +Echinococcus Ab to confirm dx
🔹While admitted, ERCP stent of obstructed biliary tree led to improved LFTs
🔹Several wks later, had excision of hydatic cyst and L hepatic lobectomy 👇
🔹Dx was initially made radiographically ➡️ Started on albendazole
🔹Later +Echinococcus Ab to confirm dx
🔹While admitted, ERCP stent of obstructed biliary tree led to improved LFTs
🔹Several wks later, had excision of hydatic cyst and L hepatic lobectomy 👇

4/Echinococcosis!
✳️4 spp cause human infection, 2 most common:
▪️E.granulosus (hydatid dz/dog tapeworm)➡️cystic echinococcosis
▪️E.multilocularis➡️alveolar
✳️Transmission: ingestion of viable eggs in contaminated food, water, soil or direct contact with animal host
✳️4 spp cause human infection, 2 most common:
▪️E.granulosus (hydatid dz/dog tapeworm)➡️cystic echinococcosis
▪️E.multilocularis➡️alveolar
✳️Transmission: ingestion of viable eggs in contaminated food, water, soil or direct contact with animal host
5/
▪️Adult E.granulosus in bowel of definitive host➡️pass eggs in feces
▪️Intermediate hosts ingest➡️egg hatch in small bowel➡️release oncosphere
▪️Oncospheres penetrate intestinal mucosa➡️migrate into organs, esp liver/lung➡️develops cyst
▪️Adult E.granulosus in bowel of definitive host➡️pass eggs in feces
▪️Intermediate hosts ingest➡️egg hatch in small bowel➡️release oncosphere
▪️Oncospheres penetrate intestinal mucosa➡️migrate into organs, esp liver/lung➡️develops cyst


6/E.granulosus
🔸Initial asx 1ary phase (may acquire as child but asx until adult)
🔸Sxs depend on size/site of cyst
🔸Usu liver (esp R lobe), then pulm (may report "salty" sputum)
🔸Cysts can rupture into biliary tree➡️biliary colic/ obstructive jaundice/cholangitis/pancreatitis
🔸Initial asx 1ary phase (may acquire as child but asx until adult)
🔸Sxs depend on size/site of cyst
🔸Usu liver (esp R lobe), then pulm (may report "salty" sputum)
🔸Cysts can rupture into biliary tree➡️biliary colic/ obstructive jaundice/cholangitis/pancreatitis
7/
🔸Majority of granulosus = single organ involvement
🔸Cysts growth is variable, but likely ~1-5cm/yr
pubmed.ncbi.nlm.nih.gov/10589894/
As for E.multilocularis,
🔸More commonly symptomatic
🔸Rarely extrahepatic
🔸Liver lesions might be more mass-like than cystic
🔸Majority of granulosus = single organ involvement
🔸Cysts growth is variable, but likely ~1-5cm/yr
pubmed.ncbi.nlm.nih.gov/10589894/
As for E.multilocularis,
🔸More commonly symptomatic
🔸Rarely extrahepatic
🔸Liver lesions might be more mass-like than cystic
8/
🚨Cyst rupture➡️fever+acute hypersensitivity rxn (including anaphylaxis): release of antigenic material + 2ary immuno rxns
📰Dx usu combo of radiology + serology
🧪Pts w/liver cysts more likely to be seropositive than lung cysts
▪️Serology sn/sp: multilocularis >> granulosus
🚨Cyst rupture➡️fever+acute hypersensitivity rxn (including anaphylaxis): release of antigenic material + 2ary immuno rxns
📰Dx usu combo of radiology + serology
🧪Pts w/liver cysts more likely to be seropositive than lung cysts
▪️Serology sn/sp: multilocularis >> granulosus
9/
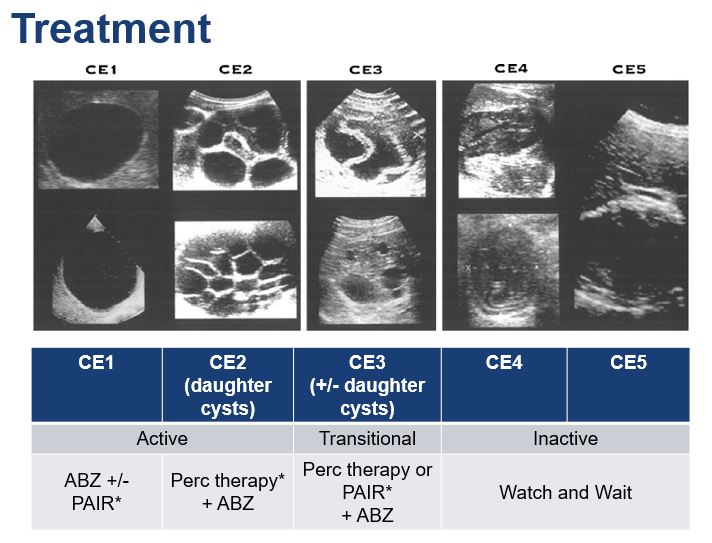
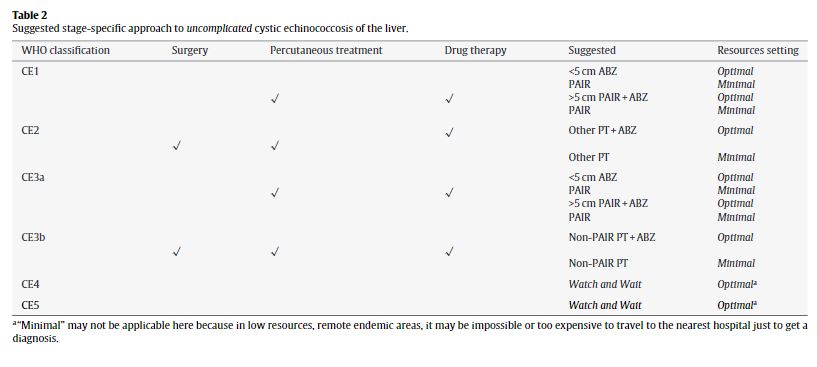
Tx depends on sxs, size/location of cysts.Can use WHO classification and treatment guidance
pubmed.ncbi.nlm.nih.gov/12606104/
pubmed.ncbi.nlm.nih.gov/19931502/
Tx options may include:
Watch & wait
Albendazole (ALB)
ALB +/- perc tx or surgery
Think about complications and whether daughter cysts
Tx depends on sxs, size/location of cysts.Can use WHO classification and treatment guidance
pubmed.ncbi.nlm.nih.gov/12606104/
pubmed.ncbi.nlm.nih.gov/19931502/
Tx options may include:
Watch & wait
Albendazole (ALB)
ALB +/- perc tx or surgery
Think about complications and whether daughter cysts
10/
🚨Important to given ALB prior/after procedures given risk of allergic rxn fr cyst rupture and/or intraperiton spillage
🔪Think surgery if complicated (rupture, biliary fistula, compression, 2ary infection or hemorrhage, mult daughter vesicles)
🪡More on percutaneous mgmt 👇
🚨Important to given ALB prior/after procedures given risk of allergic rxn fr cyst rupture and/or intraperiton spillage
🔪Think surgery if complicated (rupture, biliary fistula, compression, 2ary infection or hemorrhage, mult daughter vesicles)
🪡More on percutaneous mgmt 👇
11/
Perc options:
(1) PAIR (puncture, aspiration, injection, re-aspiration): aim to destroy germinal layer; usu ok if no daughter cysts
(2) evacuate cyst w/large-bore catheter
Risk anaphylaxis w/PAIR ~1% (improvement in fine catheters,advanced imaging)
pubmed.ncbi.nlm.nih.gov/21695106/
Perc options:
(1) PAIR (puncture, aspiration, injection, re-aspiration): aim to destroy germinal layer; usu ok if no daughter cysts
(2) evacuate cyst w/large-bore catheter
Risk anaphylaxis w/PAIR ~1% (improvement in fine catheters,advanced imaging)
pubmed.ncbi.nlm.nih.gov/21695106/


