Check out the #MINOCA section in updated NSTE-ACS guidelines at #ESCcongress
bit.ly/3bcrixp
Here is a tweetorial on #MINOCA
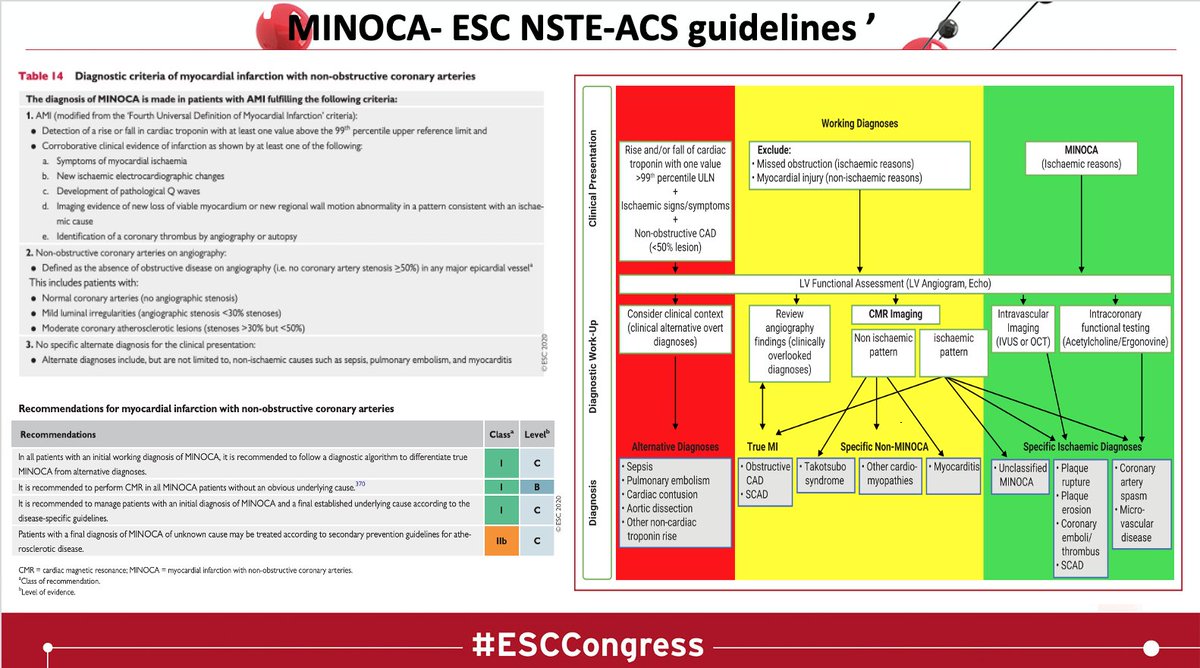
🧲Class I Recommendations🧲
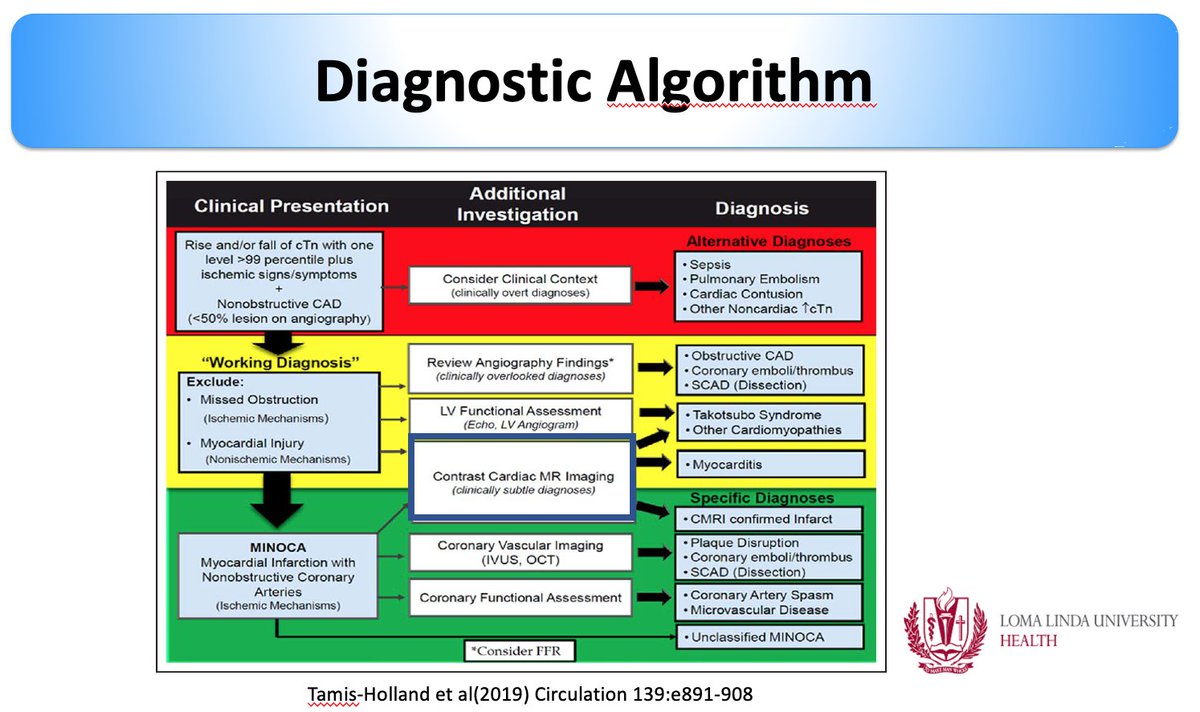
-> Use of Diagnostic algorithm
-> Use of #whyCMR
-> Use of working dx & Rx according to the underlying Dx
bit.ly/3bcrixp
Here is a tweetorial on #MINOCA
🧲Class I Recommendations🧲
-> Use of Diagnostic algorithm
-> Use of #whyCMR
-> Use of working dx & Rx according to the underlying Dx
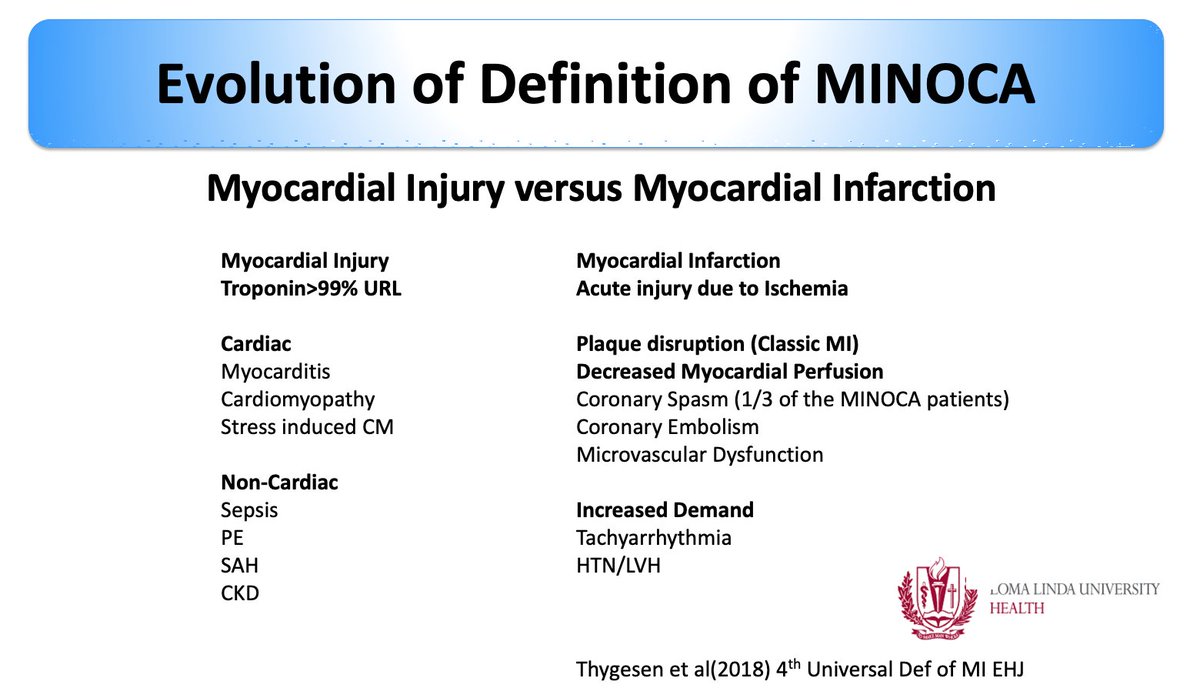
MINOCA has MI in it-> DOES the definition allows for the inclusion of non-ischemic causes of troponin elevation?
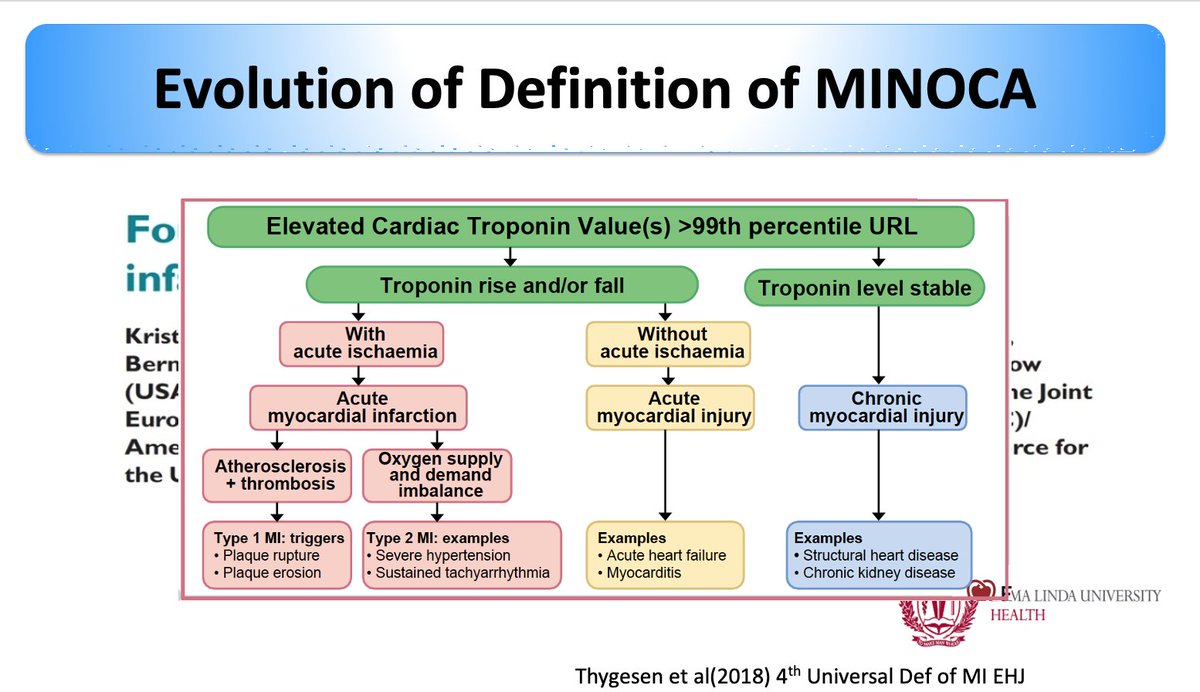
Given this limitation of the troponin bioassay, the “Fourth 4th Universal of MI" defined Injury from infarction
INJURY IS NECROSIS WITHOUT ISCHEMIA!
#ESCCongress
Given this limitation of the troponin bioassay, the “Fourth 4th Universal of MI" defined Injury from infarction
INJURY IS NECROSIS WITHOUT ISCHEMIA!
#ESCCongress
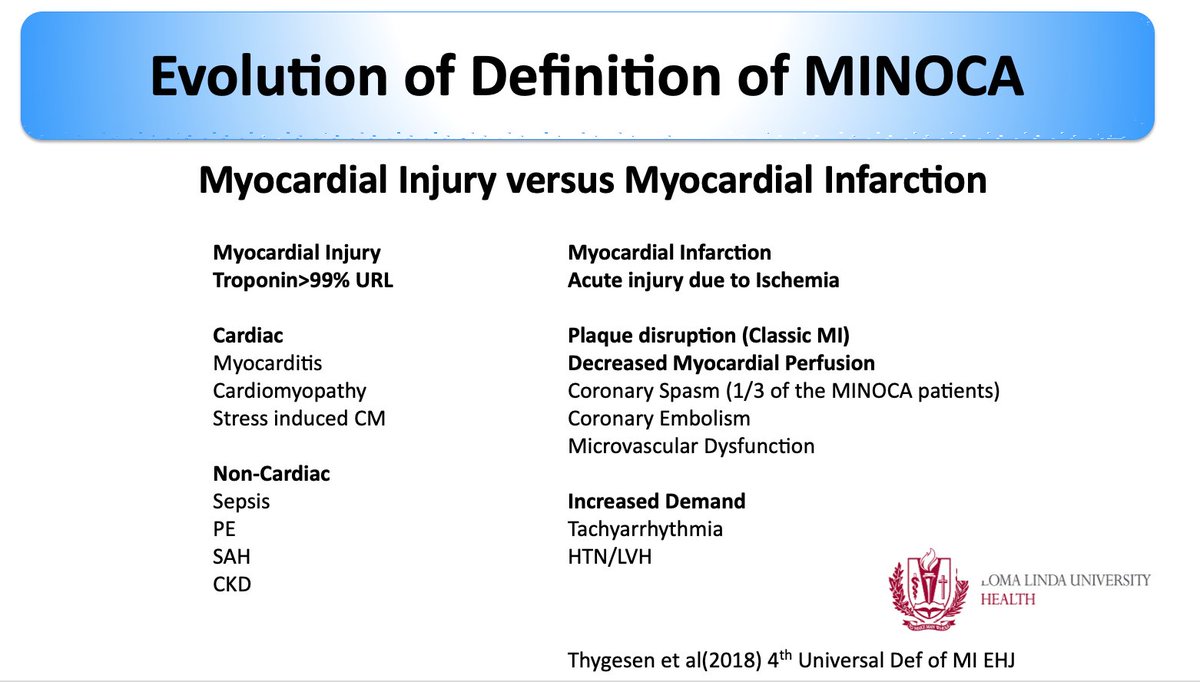
The hallmark of myocardial injury ⬆️ troponin, However, these entities differ conceptually
▶️ myocardial injury = nonischemic mechanisms of myocyte injury (eg, myocarditis),
▶️MI = ischemic mechanisms (eg,
plaque disruption or supply-demand mismatch).
#ESCCongress
▶️ myocardial injury = nonischemic mechanisms of myocyte injury (eg, myocarditis),
▶️MI = ischemic mechanisms (eg,
plaque disruption or supply-demand mismatch).
#ESCCongress
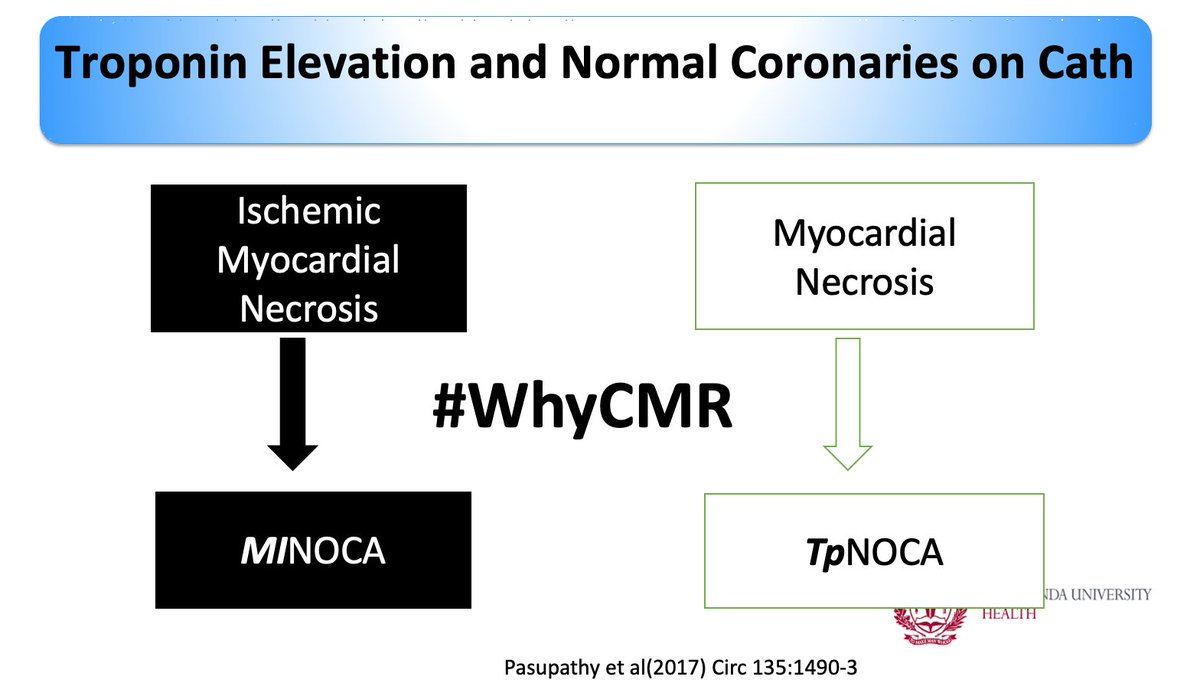
Limitation of the definition of #MINOCA has been described before!
bit.ly/3jn81Mu talks about TpNOCA to be inclusive of nonischemic causes
Important to acknowledge
MINOCA or TpNOCA - WORKING DIAGNOSIS
#whyCMR is the KEY to identify the diagnosis!
#ESCcongress
bit.ly/3jn81Mu talks about TpNOCA to be inclusive of nonischemic causes
Important to acknowledge
MINOCA or TpNOCA - WORKING DIAGNOSIS
#whyCMR is the KEY to identify the diagnosis!
#ESCcongress
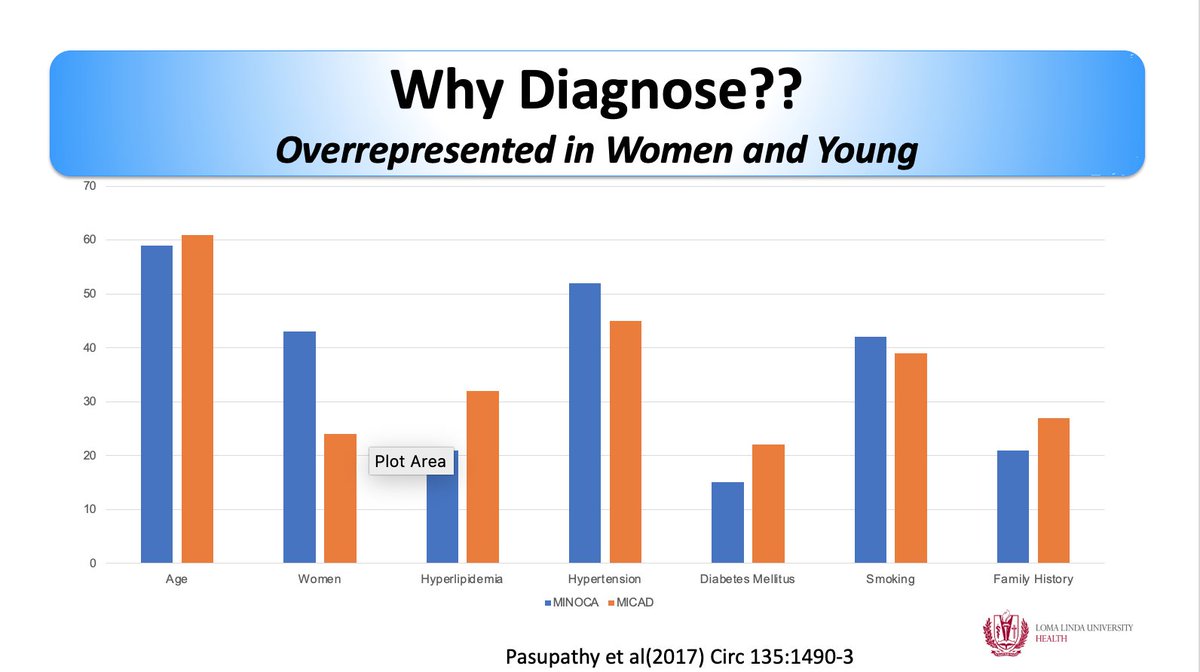
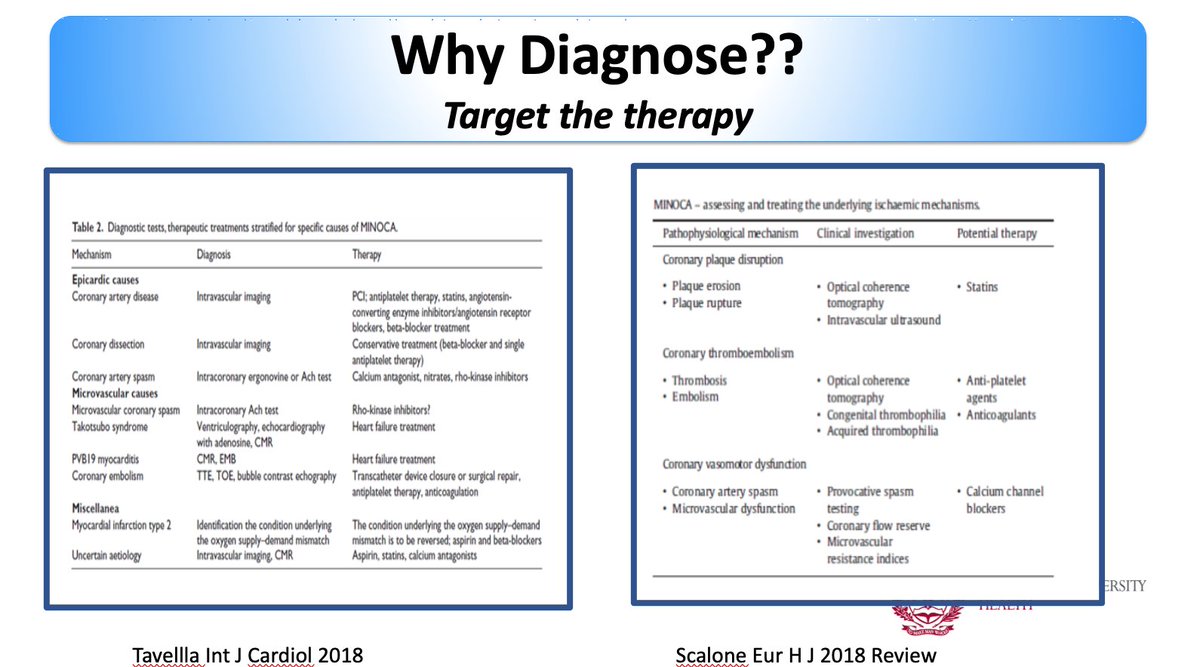
@chiarabd @afshinfarzan @VicFerrariMD @LiliaSierra2 @CardioimagenINC @mmamas1973 @s_gati @MarcDweck @cshenoy3 @denisamuraru why Diagnose #MINOCA?
▶️ Overrepresentation in women and young
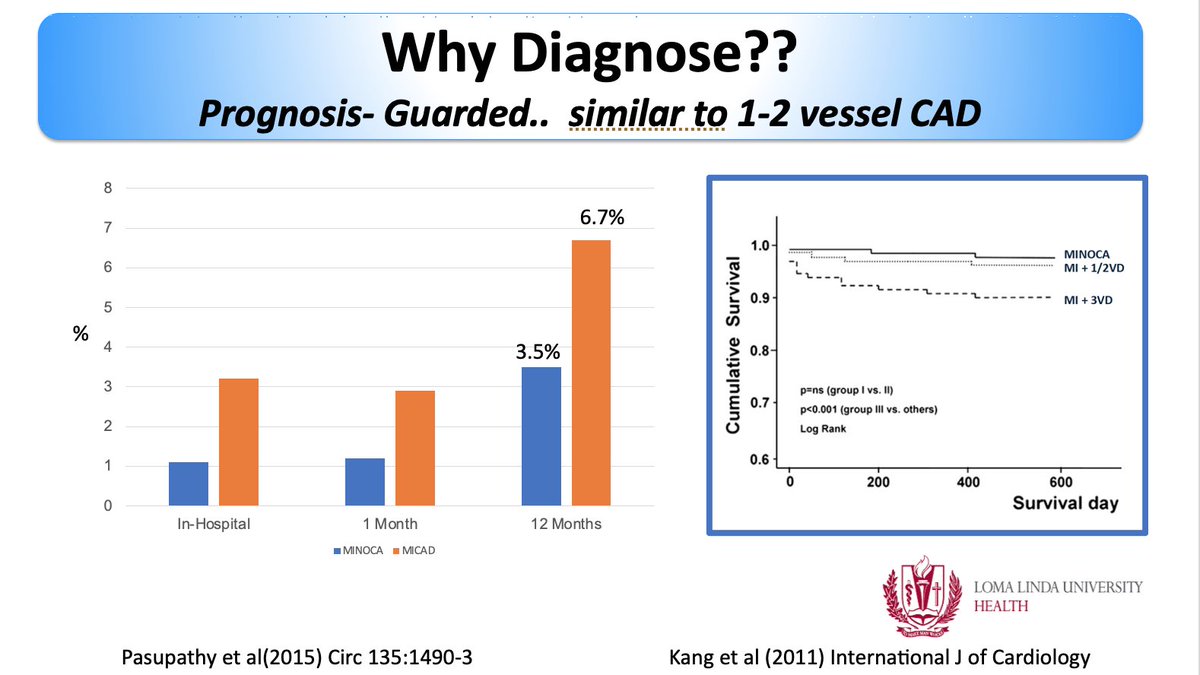
▶️ Prognosis guarded - Similar to 1-2 vessel CAD
▶️ To, Target the therapy (Now class I recommendation to do so!
#ESCCongress
▶️ Overrepresentation in women and young
▶️ Prognosis guarded - Similar to 1-2 vessel CAD
▶️ To, Target the therapy (Now class I recommendation to do so!
#ESCCongress
Once #whyCMR confirms #MINOCA
Now the guidelines recommend the use of #intracoronary acetylcholine can be performed when the coronary or microvascular spasm is suspected
#IVUS or #OCT #radialfirst valuable ▶️ for thrombus, plaque rupture or erosion, or SCAD
#ESCCongress
Now the guidelines recommend the use of #intracoronary acetylcholine can be performed when the coronary or microvascular spasm is suspected
#IVUS or #OCT #radialfirst valuable ▶️ for thrombus, plaque rupture or erosion, or SCAD
#ESCCongress
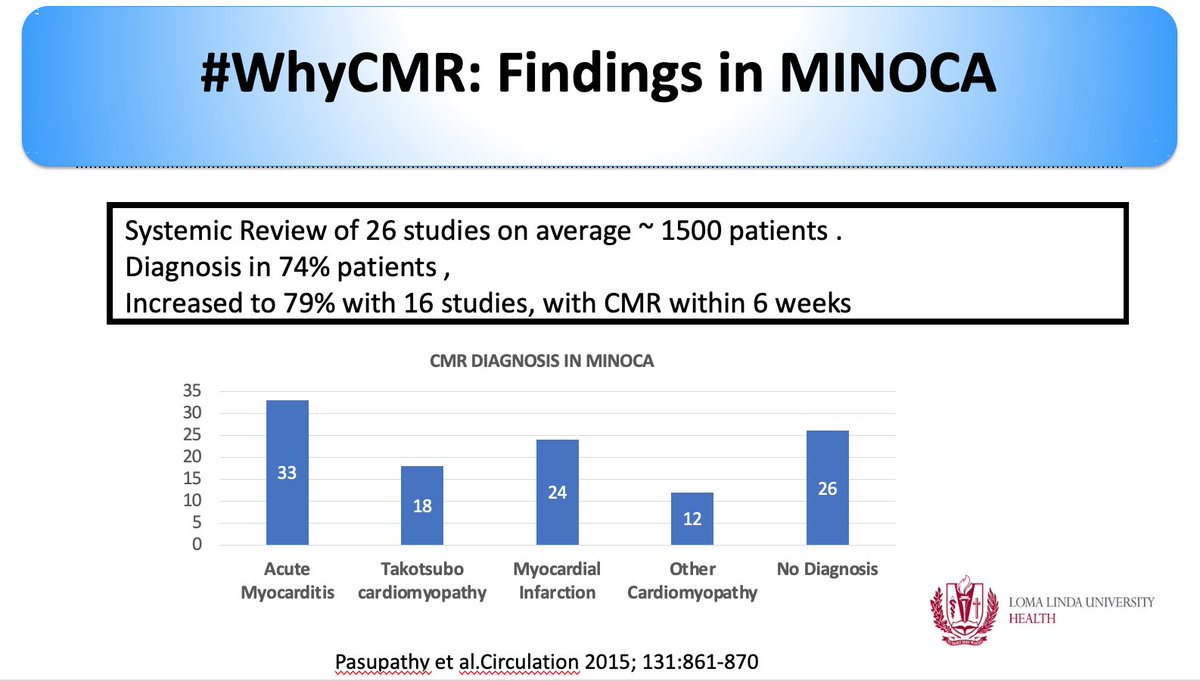
Guidelines cite this 📰 -> meta-analysis of 26 CMR 📰
#myocarditis as the leading cause on #whyCMR in patients with working diagnosis of #MINOCA
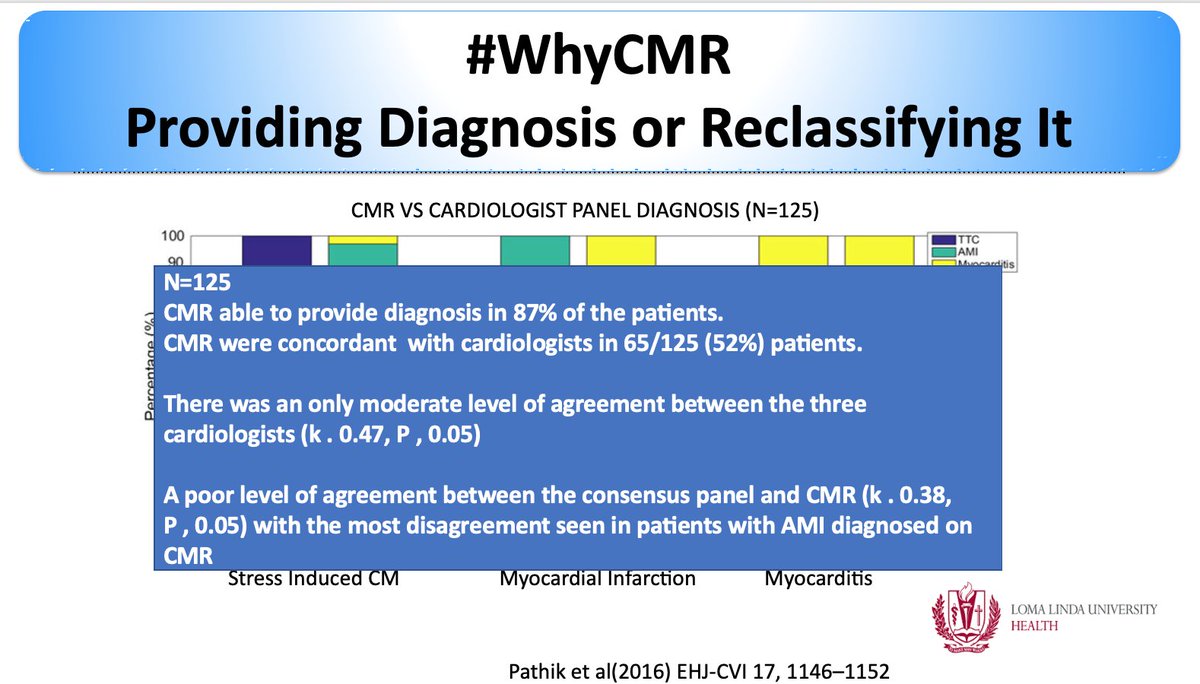
🧲 Since then many #whyCMR studies in the literature.
🧲#whyCMR able to identify etiology ~ 87% of the cases
#ESCCongress
#myocarditis as the leading cause on #whyCMR in patients with working diagnosis of #MINOCA
🧲 Since then many #whyCMR studies in the literature.
🧲#whyCMR able to identify etiology ~ 87% of the cases
#ESCCongress
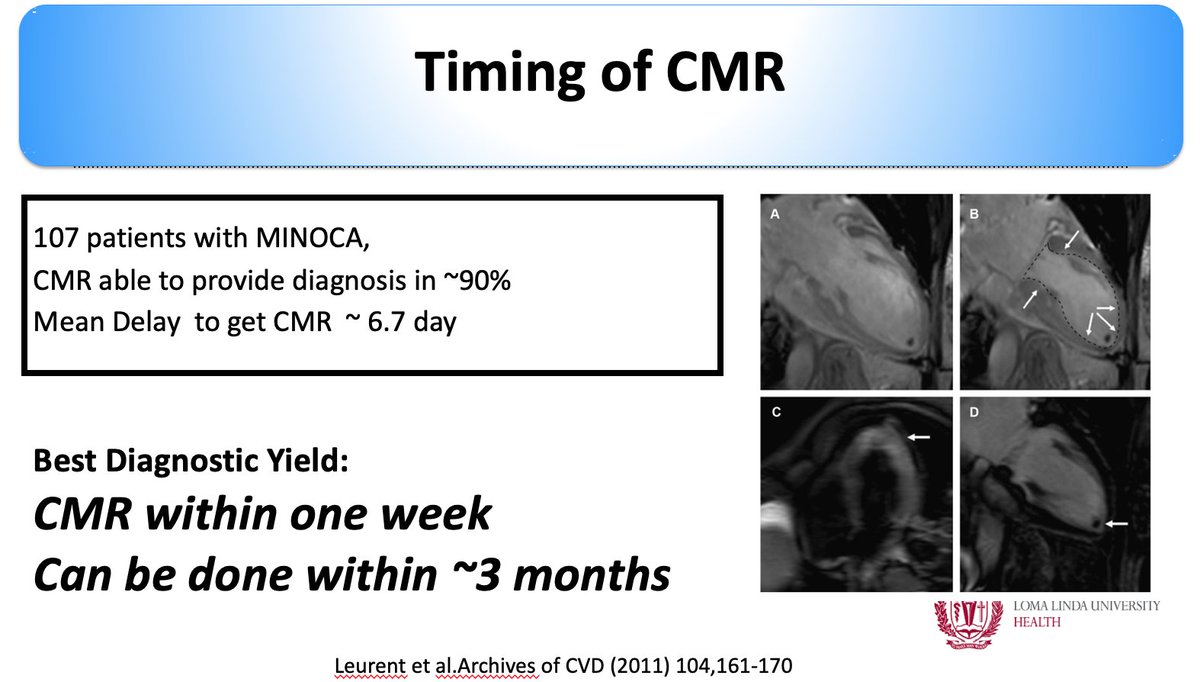
Q: when to do #whyCMR in cases of #MINOCA?
The guidelines don't touch upon this however literature suggest best diagnostic yield within a week -- However robust diagnostic ability maintained up to ~3 months
(Can be done, OUTPATIENT)
#ESCCongress
The guidelines don't touch upon this however literature suggest best diagnostic yield within a week -- However robust diagnostic ability maintained up to ~3 months
(Can be done, OUTPATIENT)
#ESCCongress
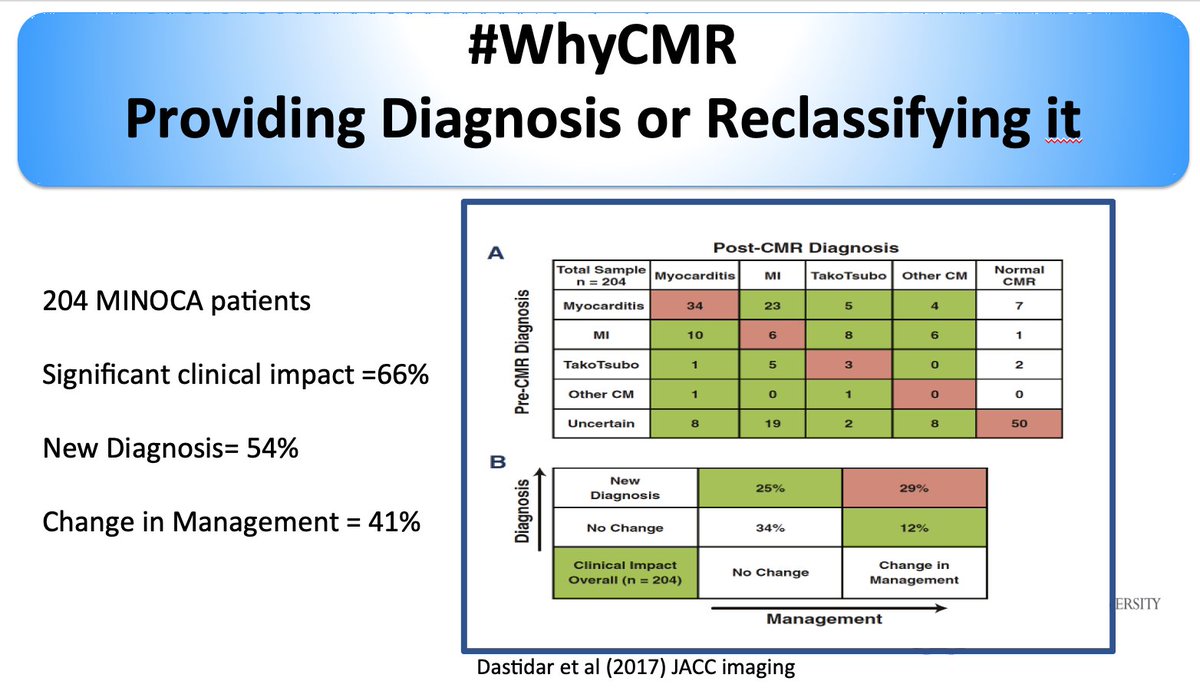
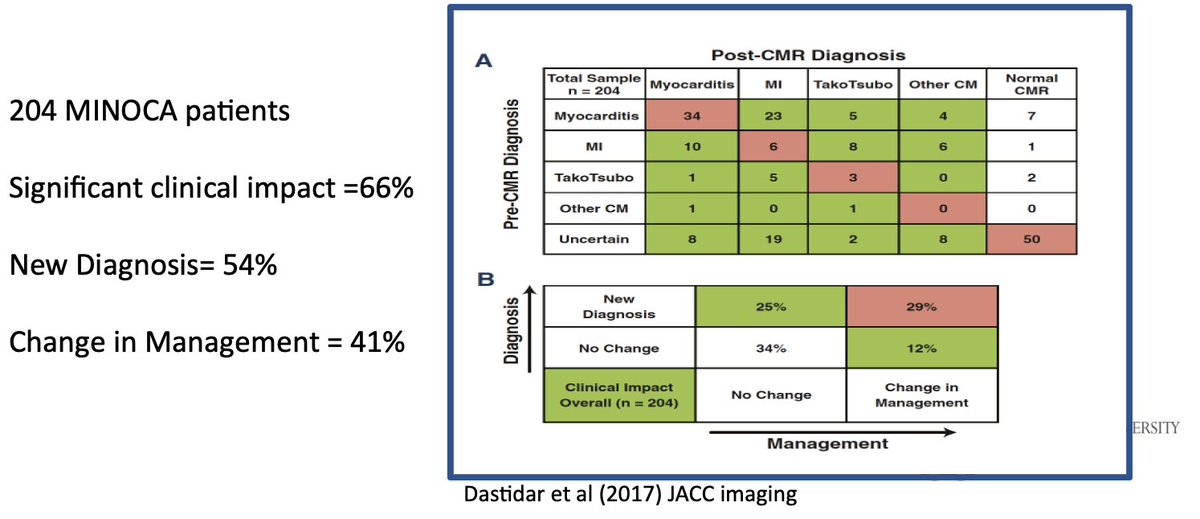
Q: Diagnosis may be clearcut why do #whyCMR
▶️Prognostic data to indicate the change in the management with #whyCMR great study by @chiarabd
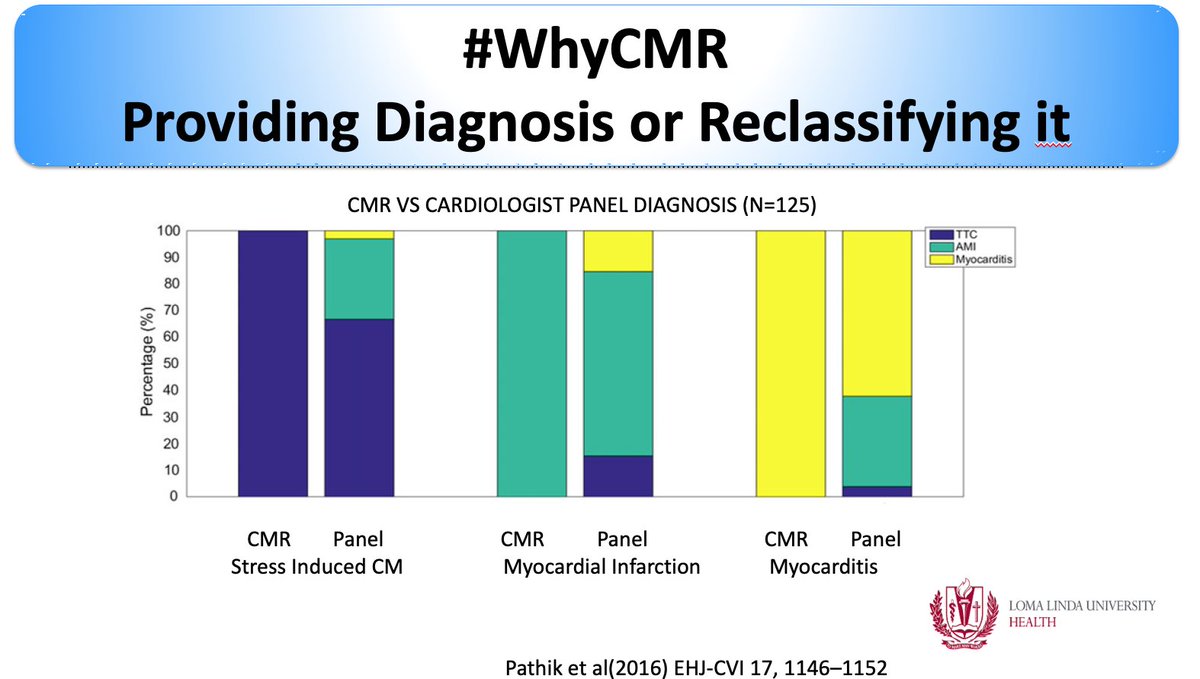
▶️ Also the poor level of agreement pre-#whyCMR diagnosis amongst clinicians
#ESCCongress
▶️Prognostic data to indicate the change in the management with #whyCMR great study by @chiarabd
▶️ Also the poor level of agreement pre-#whyCMR diagnosis amongst clinicians
#ESCCongress
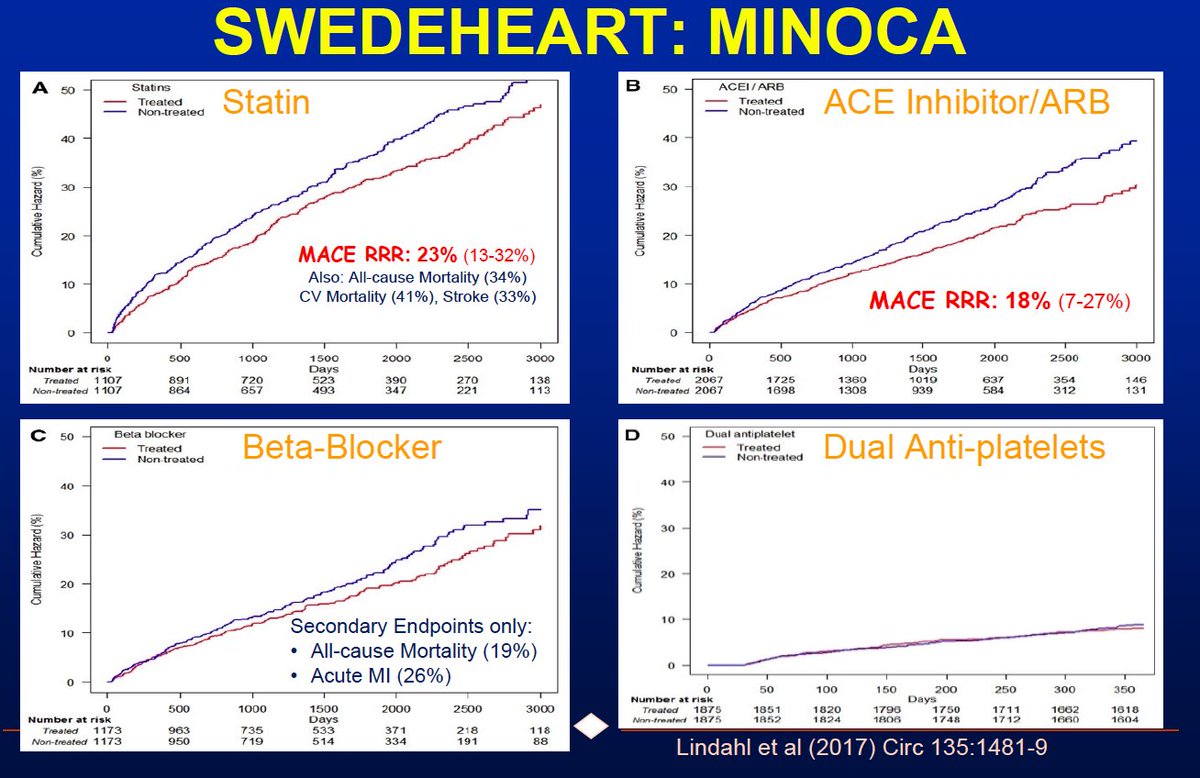
What about the Rx of #MINOCA?
Guideline document cite this paper(1st slide)
▶️ limited date on Dual Antiplatelet
▶️ Use of ACE, BB, Statin based on the registry data (this registry didn't apply the current MINOCA criteria
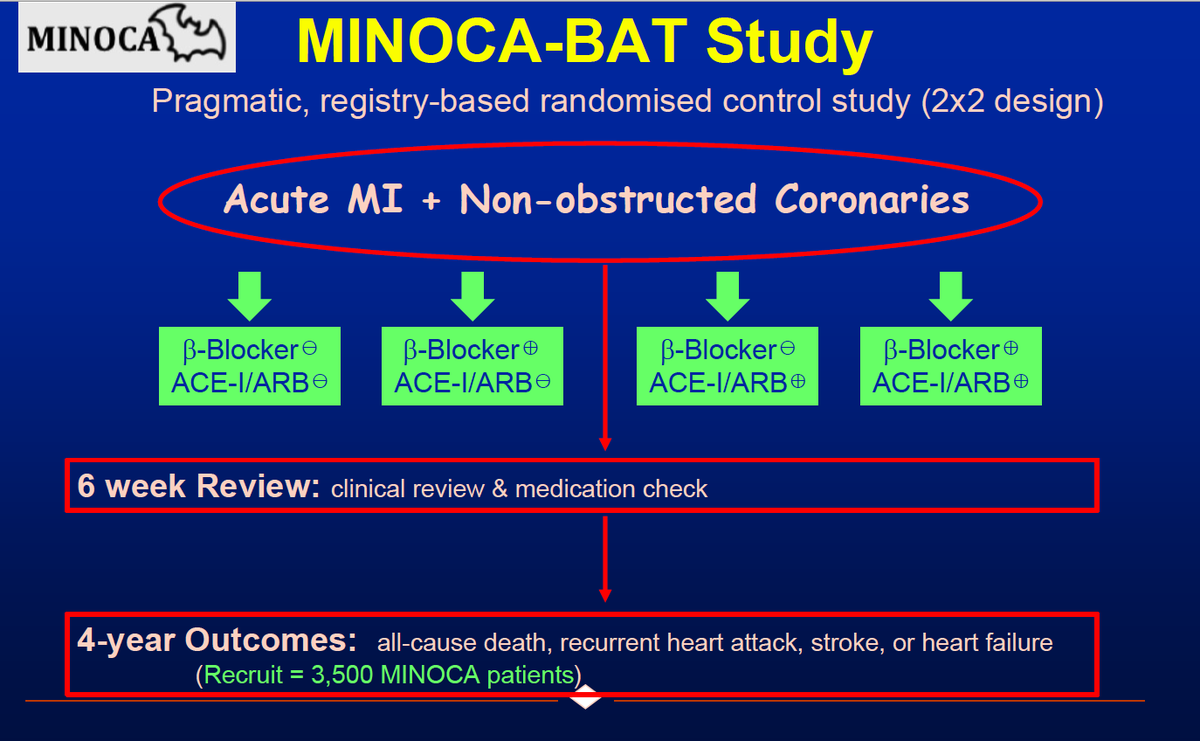
MINOCA-BAT awaited!
#ESCCongress
Guideline document cite this paper(1st slide)
▶️ limited date on Dual Antiplatelet
▶️ Use of ACE, BB, Statin based on the registry data (this registry didn't apply the current MINOCA criteria
MINOCA-BAT awaited!
#ESCCongress