1/#Morningreport @SinaiBmoreIMRes
featured a young patient presenting with abdominal pain X 2 weeks with a serum K=2.8.
There was also increased urinary frequency
some weakness and fatigue during the past 2 weeks
#DDX #MedTwitter #medstudents #FOAMed
featured a young patient presenting with abdominal pain X 2 weeks with a serum K=2.8.
There was also increased urinary frequency
some weakness and fatigue during the past 2 weeks
#DDX #MedTwitter #medstudents #FOAMed
2/The DDX for Hypokalemia requires consideration of a 3 pronged approach: 1)Decreased intake 2)Renal and GI losses and 3) IC shifts. 

3/For the workup: Spot urine potassium and 24 hour urinary Potassium suggested urinary K wasting.
[UK] high (>40 mEq/L) =renal K loss
TTKG of 9 was concerning for renal potassium wasting
In hypokalemia (K⁺ <3.5 mEq/L), the TTKG > 7 suggests renal K wasting.
[UK] high (>40 mEq/L) =renal K loss
TTKG of 9 was concerning for renal potassium wasting
In hypokalemia (K⁺ <3.5 mEq/L), the TTKG > 7 suggests renal K wasting.

4/In this patient, there was also metabolic alkalosis and volume depletion with high urine Cl making a case for suspected Gitelman or Barrter syndrome.
We can tell the difference with a UCa. Low spot Ca:Cr ratio suggests a DX of Gitelman syndrome.
We can tell the difference with a UCa. Low spot Ca:Cr ratio suggests a DX of Gitelman syndrome.

4/#Pearl
Manifestations of hypoK: vomiting, diarrhea, ileus, anorexia muscle weakness including respiratory muscles,
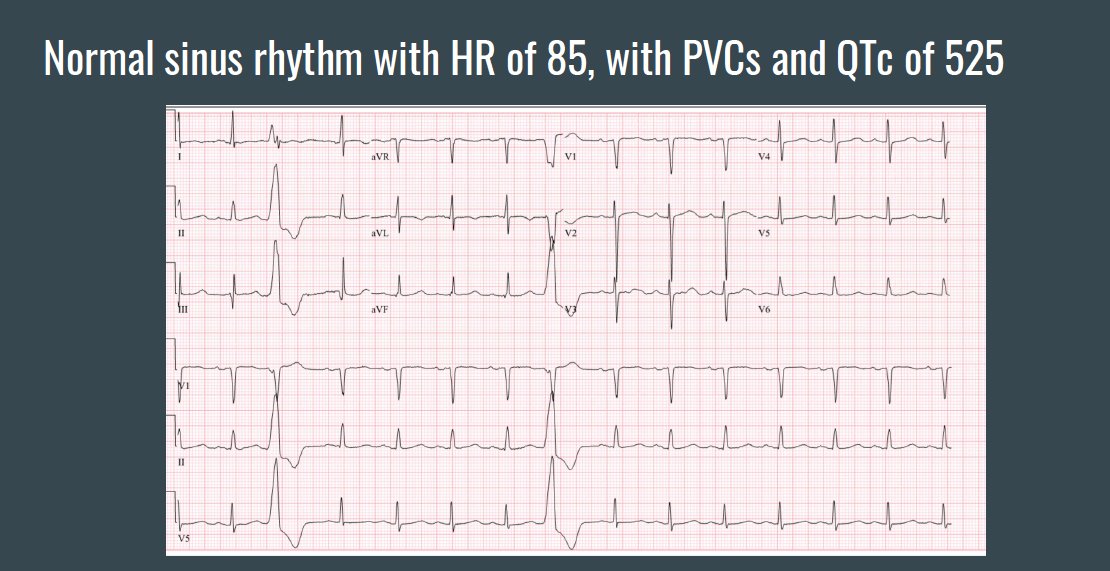
ECG changes: PACs, sinus bradycardia, ST depression, decrease in the amplitude of the T wave, and U waves in the lateral precordial leads. QT prolongation
Manifestations of hypoK: vomiting, diarrhea, ileus, anorexia muscle weakness including respiratory muscles,
ECG changes: PACs, sinus bradycardia, ST depression, decrease in the amplitude of the T wave, and U waves in the lateral precordial leads. QT prolongation

5/#Pearl
Note: A normal individual can, in the presence of potassium depletion that is not due to urinary losses, lower urinary potassium excretion below 25 to 30 mEq per day on a 24-hour urine
Note: A normal individual can, in the presence of potassium depletion that is not due to urinary losses, lower urinary potassium excretion below 25 to 30 mEq per day on a 24-hour urine
6/#Pearl: The most common causes of hypokalemia are either GI (vomting, diarrhea) or Urine wasting (eg. Diuretic)

7/#Pearl: assess potassium excretion: 24-hour urine collection or alternatively with potassium-to-creatinine ratio on a spot urine are alternatives.
-can check The TTKG: During hypokalemia (K⁺ <3.5 mEq/L), the TTKG should be <3; greater values suggest renal K wasting
-can check The TTKG: During hypokalemia (K⁺ <3.5 mEq/L), the TTKG should be <3; greater values suggest renal K wasting

8/Check out the most recent hypokalemia tweetorials by @RezidentMD.
https://twitter.com/RezidentMD/status/1299832379679354880
https://twitter.com/RezidentMD/status/1300127192345702405
• • •
Missing some Tweet in this thread? You can try to
force a refresh