1/ In medicine, we get to eat humble pie time and time again. The vast amount of knowledge necessary can be a daunting task and what we learn isn't necessarily what we may see in the clinical realm. You can almost say there is an atypical presentation for everything. 

2/ This leads to our case, on consults we come across a elderly pt with confusion and psychosis.
Normal Temp and RR: 18 and Low normal BP
Clinically dry with labs:
Normal Albumin and Normal gap.
Normal Temp and RR: 18 and Low normal BP
Clinically dry with labs:
Normal Albumin and Normal gap.

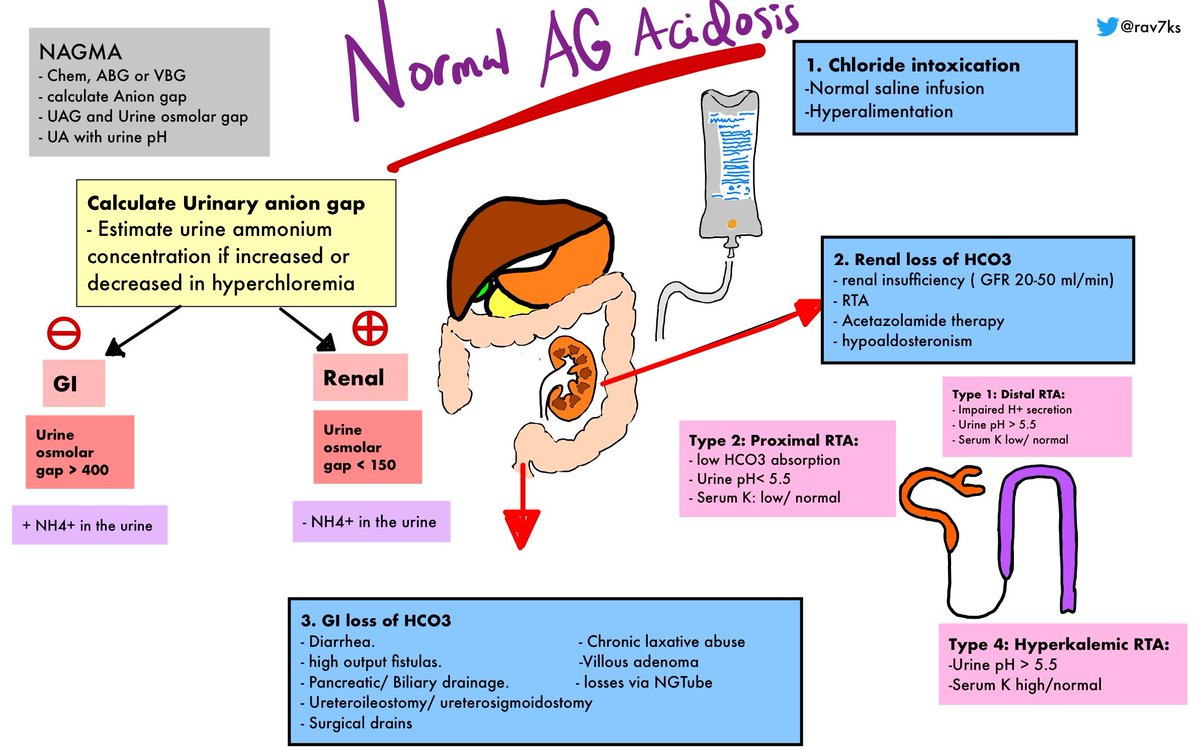
3/ Her NAGMA was not competely explained by the hyperchloremia but this could be a contributor.
The next step was to pursue a UAG.
Her ABG was unremarkable and a run through of causes of NAGMA came up empty.
The next step was to pursue a UAG.
Her ABG was unremarkable and a run through of causes of NAGMA came up empty.
4/However, with ASA on the list of this patient's medications. We decided to order a level along with a battery of other tests to find the needle in the haystack that could explain the metabolic encephalopathy.
Lo and Behold the level returned back CRITICALLY HIGH.
Lo and Behold the level returned back CRITICALLY HIGH.

5/ Wait a minute we all said !
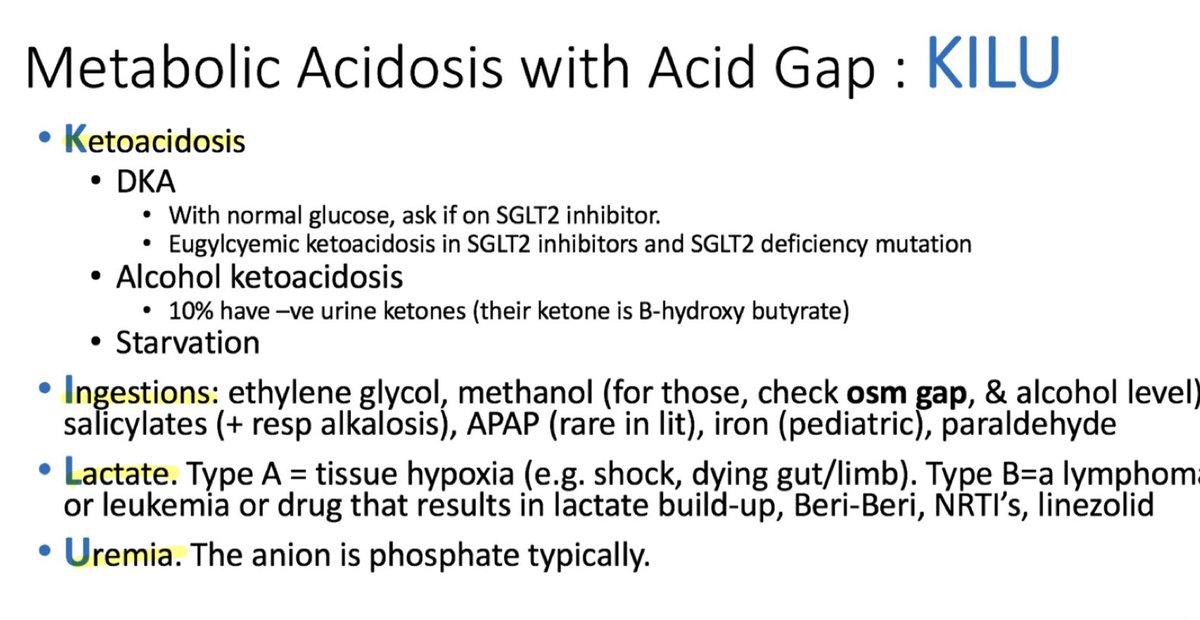
"This does not fit our illness script for ASA toxicity. This is absolutely incorrect especially with the lack of HAGMA when running through KILU @UnremarkableLab "
"This does not fit our illness script for ASA toxicity. This is absolutely incorrect especially with the lack of HAGMA when running through KILU @UnremarkableLab "
6/In addition, the patient did not manifest with N/V,Tachypnea, hyperpnea, Tinnitus, Nausea/vomiting: or Hyperthermia. Only confusion/Psychosis.

7/The mechanism for HAGMA in ASA overdose is due to salicylic acid uncoupling oxidative phosphorylation, leading to accumulation of lactic acid and pyruvic acid, causing a primary elevated anion gap metabolic acidosis.
Courtesy of REBELEM
Courtesy of REBELEM

8/ However, salicylate can interfere with lab assay for chloride, causing falsely elevated chloride and making it appear as though anion gap is normal.
In our case, the Cl was elevated and hence the AG was calculated to be normal.
In our case, the Cl was elevated and hence the AG was calculated to be normal.
9/Key points:
a. 20% of patients have a hyperchloremic
normal anion-gap acidosis
b.Increased excretion of bicarbonate accompanied
by retention of chloride is a compensatory response
of the kidney to respiratory alkalosis.
nejm.org/doi/full/10.10…
a. 20% of patients have a hyperchloremic
normal anion-gap acidosis
b.Increased excretion of bicarbonate accompanied
by retention of chloride is a compensatory response
of the kidney to respiratory alkalosis.
nejm.org/doi/full/10.10…
10/
c.Urinary excretion of Na and K
salts of organic acids is the equivalent of
losing NaHCO3 from the body. The
contraction of ECF volume
signals renal retention of dietary sodium chloride
c.Urinary excretion of Na and K
salts of organic acids is the equivalent of
losing NaHCO3 from the body. The
contraction of ECF volume
signals renal retention of dietary sodium chloride
11/
d.concomitant ingestion of
bromide-containing compounds can cause
false elevation in the Cl level, since
both bromide and chloride are halides
d.concomitant ingestion of
bromide-containing compounds can cause
false elevation in the Cl level, since
both bromide and chloride are halides
12/
e.Increased plasma salicylate level can cause
autoanalyzers to falsely report an increased
plasma chloride level, leading to an erroneously
low or even negative value for the anion gap.
e.Increased plasma salicylate level can cause
autoanalyzers to falsely report an increased
plasma chloride level, leading to an erroneously
low or even negative value for the anion gap.
13/
Consider salicylate poisoning inspite of a NAGMA in the presence of hyperchloremia.
Another situation where ASA overdose that we've seen is overuse of Pepto-Bismol which contains salicylate (8.7 mg per milliliter) in the form of bismuth subsalicylate.
Consider salicylate poisoning inspite of a NAGMA in the presence of hyperchloremia.
Another situation where ASA overdose that we've seen is overuse of Pepto-Bismol which contains salicylate (8.7 mg per milliliter) in the form of bismuth subsalicylate.

14/
Getting back to humble pie.
In actuality, it is not a pie that we would want to consume. Humbles are the insides of an animal, especially a deer, used as food. It remains a vanished dish of the medieval past.
For now it remains an expression when we are proved wrong.
Getting back to humble pie.
In actuality, it is not a pie that we would want to consume. Humbles are the insides of an animal, especially a deer, used as food. It remains a vanished dish of the medieval past.
For now it remains an expression when we are proved wrong.

• • •
Missing some Tweet in this thread? You can try to
force a refresh