Why is stopping a #SARSCoV2 vaccine trial early such a bad idea?
A proper clinical trial is statistically powered to make a call at its completion
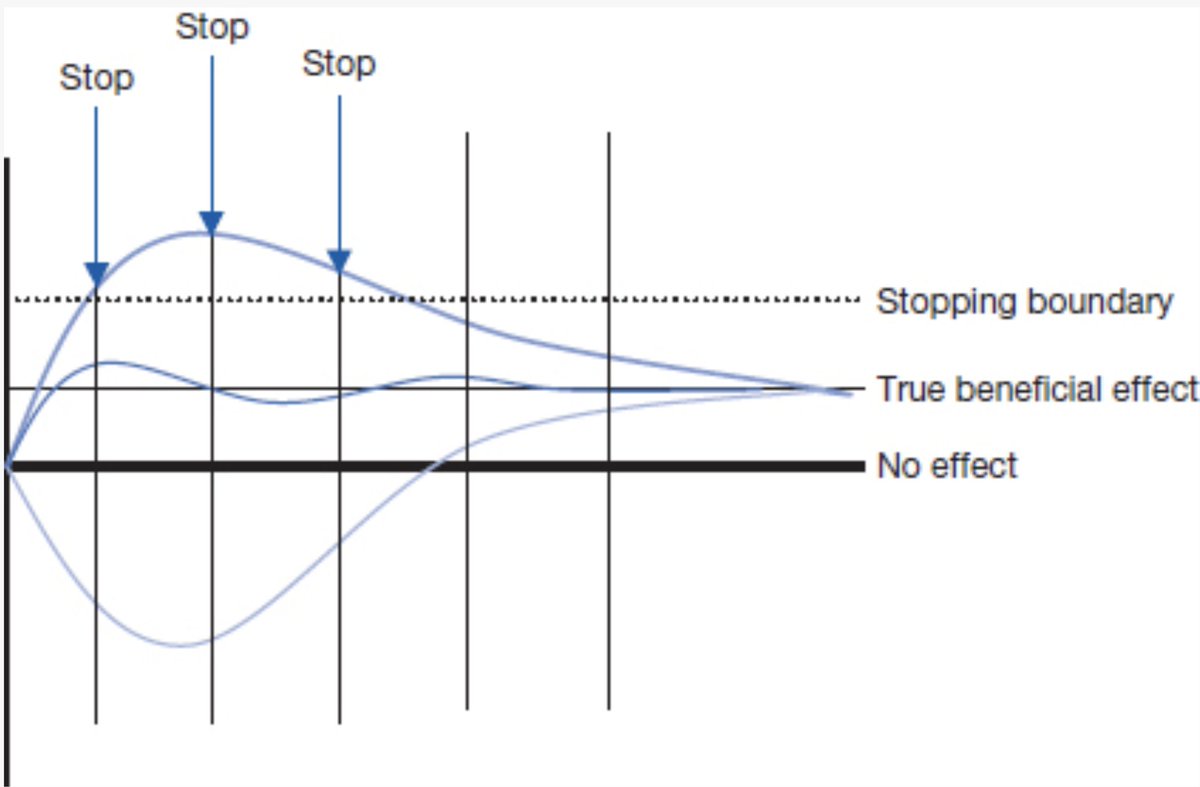
There's wobble, random chance, in events during a trial
The true beneficial effect has turned out less in some trials stopped early
A proper clinical trial is statistically powered to make a call at its completion
There's wobble, random chance, in events during a trial
The true beneficial effect has turned out less in some trials stopped early
The trials are reportedly powered to detect 50% efficacy w/ a lower 95% CI of 30%. That's not nearly as high as ideal
Stopping early:
— could even exaggerate that
— could impact other placebo-controlled trials
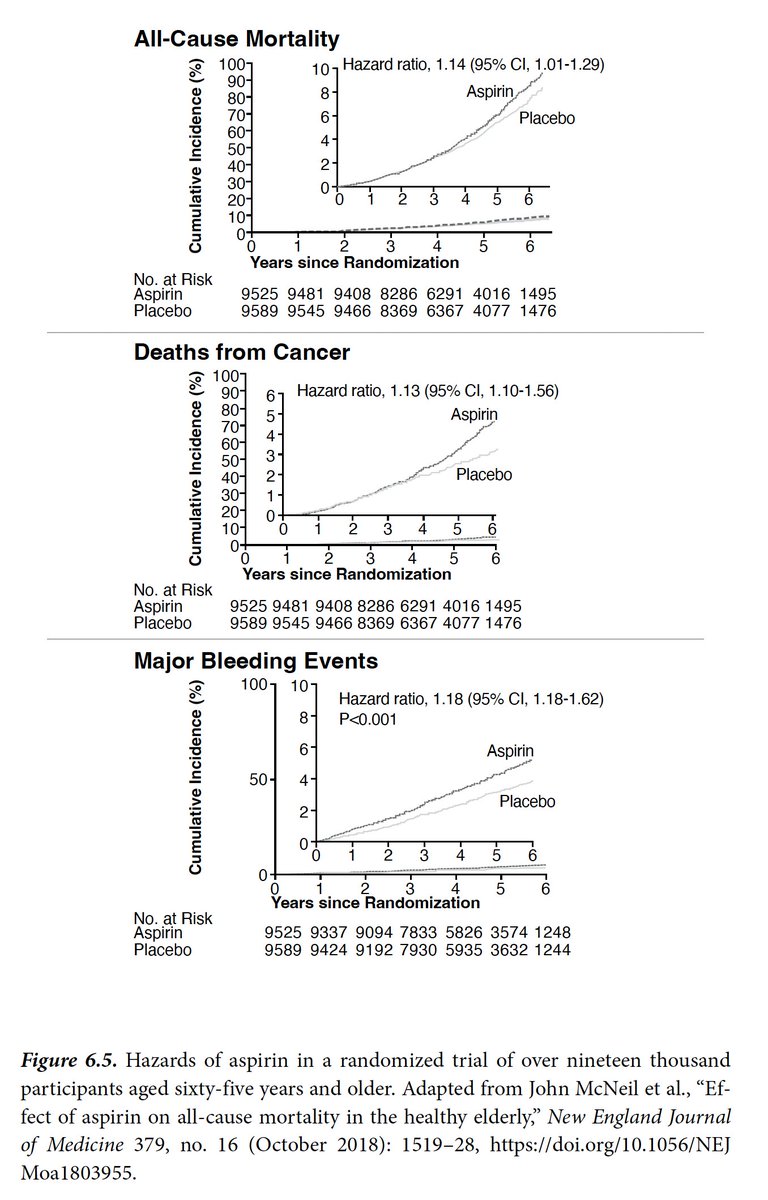
— could also miss relatively rare but important adverse safety events
Stopping early:
— could even exaggerate that
— could impact other placebo-controlled trials
— could also miss relatively rare but important adverse safety events
The @pfizer CEO again today asserted they will know by the end of October whether their vaccine w/ @BioNTech_Group works @FaceTheNation
cbsnews.com/news/covid-vac…
That can only be determined by stopping the trial early.
And they're not releasing their stopping rules.
It's all wrong
cbsnews.com/news/covid-vac…
That can only be determined by stopping the trial early.
And they're not releasing their stopping rules.
It's all wrong
• • •
Missing some Tweet in this thread? You can try to
force a refresh