@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 1/ 35 yo F panUC on IFX 10mg q4wk, admitted with abdo pain, hematochezia, malaise. T 39 BP 95/63 HR 110 FCP 900 mcg/g. Abdo distended, TTP; CT: colonic wall thickening+edematous mucosa. Cdiff neg; WBC 15, Hb 6. No improvement despite IVCS+Abx. Which surgery is indicated #B2BPoll
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 2/ Indications for colectomy in UC:
📌Elective:
📍UC refractory to medical Rx
📍Steroid-dependant UC
📍Unresectable dysplasia, CA
📍Complications from medical Rx
📌Emergency:
📍Toxic megacolon
📍Fulminant colitis
📍Perforation
📍Severe Bleeding
📌Elective:
📍UC refractory to medical Rx
📍Steroid-dependant UC
📍Unresectable dysplasia, CA
📍Complications from medical Rx
📌Emergency:
📍Toxic megacolon
📍Fulminant colitis
📍Perforation
📍Severe Bleeding

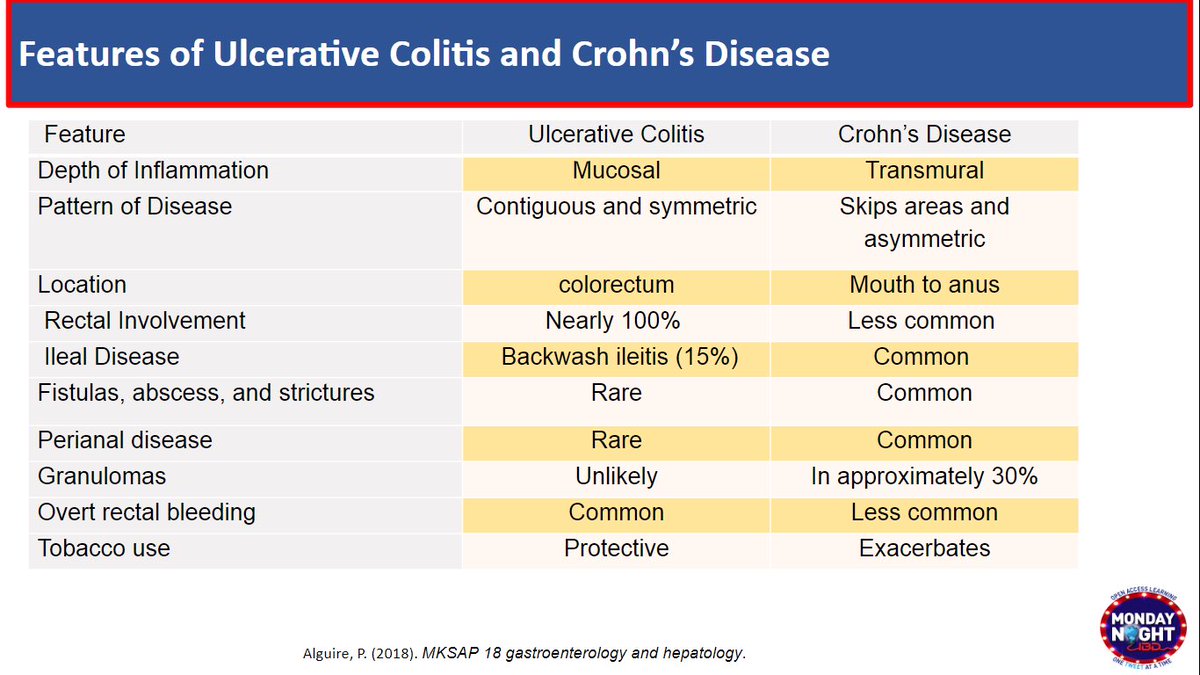
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 3/ What is a toxic megacolon?
🔺Transverse colon > 6cm
🔺AND one:
T>101.5° F
HR> 120
WBC>10.5
anemia
🔺AND one:
Dehydration
altered mental status
electrolyte abnormality
hypotension
💡Recall our #B2B tweetorial on ASUC👇🏽👇🏽👇🏽
🔺Transverse colon > 6cm
🔺AND one:
T>101.5° F
HR> 120
WBC>10.5
anemia
🔺AND one:
Dehydration
altered mental status
electrolyte abnormality
hypotension
💡Recall our #B2B tweetorial on ASUC👇🏽👇🏽👇🏽
https://twitter.com/mjayoushe/status/1279430539783606273
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 4/ What is Fulminant colitis?
🔺> 10 BM/day
Continuous bleeding
Abdominal pain+ distention
🔺AND acute, severe toxic symptoms (see 👆🏼👆🏼👆🏼)
🔺> 10 BM/day
Continuous bleeding
Abdominal pain+ distention
🔺AND acute, severe toxic symptoms (see 👆🏼👆🏼👆🏼)
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 5/ 🏁Emergency ✂️
📌Subtotal Colectomy+ ileostomy+rectum in place
📌After pt recovered, nutrition optimized,off CS,option to complete proctectomy &end-ileostomy or 3-stage pouch
📌In🤰:Turnbull-Blowhole colostomy: colostomy for colonic decompression+loop ileostomy for💩passage
📌Subtotal Colectomy+ ileostomy+rectum in place
📌After pt recovered, nutrition optimized,off CS,option to complete proctectomy &end-ileostomy or 3-stage pouch
📌In🤰:Turnbull-Blowhole colostomy: colostomy for colonic decompression+loop ileostomy for💩passage
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 6/ What happens to the rectum left in place?
🔺Hartman pouch: the proximal end of rectum is stapled off
🔺Or rectosigmoid left is long enough to create a mucous fistula= ostomy to the skin to drain mucus/gas & prevent buildup
🔺Hartman pouch: the proximal end of rectum is stapled off
🔺Or rectosigmoid left is long enough to create a mucous fistula= ostomy to the skin to drain mucus/gas & prevent buildup
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 7/ 🔑Avoid “going in the pelvis” (proctectomy, IPAA construction) in sick patients
🔺Sick= severe active disease, steroids, malnourished, septic, hemodyn unstable
🔺↑ Risk anastomotic leak , pelvic sepsis
🔺↑ Risk pouch failure long term
🔺Sick= severe active disease, steroids, malnourished, septic, hemodyn unstable
🔺↑ Risk anastomotic leak , pelvic sepsis
🔺↑ Risk pouch failure long term
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 8/ 🔺Diverting ileostomy used to be performed for emergent Sx in fulminant colitis
🔺Colon was not resected--> perforation risk and bleeding continued !!
🔺Mortality up to 70% !
🔺Not an optimal option!
🔺Colon was not resected--> perforation risk and bleeding continued !!
🔺Mortality up to 70% !
🔺Not an optimal option!
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 9/ 🏁Elective ✂️→
💡2 stages✂️:
1- Total proctocolectomy (TPC) + ileal pouch anal anastomosis (IPAA)+ ileostomy
2- ostomy takedown
💡3 stages✂️:
1- Total colectomy (TAC)+ileostomy
2- proctectomy+IPAA+ ileostomy
3- ileostomy take down
💡2 stages✂️:
1- Total proctocolectomy (TPC) + ileal pouch anal anastomosis (IPAA)+ ileostomy
2- ostomy takedown
💡3 stages✂️:
1- Total colectomy (TAC)+ileostomy
2- proctectomy+IPAA+ ileostomy
3- ileostomy take down

@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 10/ Remember why we create a #pouch #IPAA #Jpouch ?
🔺After colon + rectum✂️we need to recreate a reservoir for💩
🔺SB lumen size << rectum lumen
🔺End of SB looped in J shape & lumen “opened+sutured” together
🔺Pouch lumen now x2 SB lumen
🔺Pouch🧷🧶to anus = IPAA
🔺After colon + rectum✂️we need to recreate a reservoir for💩
🔺SB lumen size << rectum lumen
🔺End of SB looped in J shape & lumen “opened+sutured” together
🔺Pouch lumen now x2 SB lumen
🔺Pouch🧷🧶to anus = IPAA
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 11/ 🏁❌Not everyone is a candidate for IPAA
🔺Multiple medical comorbidities
🔺HGD/CA of distal rectum
🔺Anal canal requiring XRT and/or excision
🔺Fecal incontinence
🔺Older age (poor sphincter)
🔺Abdominal obesity
🔺Fertility preservation
Options 👇🏽
🔺Multiple medical comorbidities
🔺HGD/CA of distal rectum
🔺Anal canal requiring XRT and/or excision
🔺Fecal incontinence
🔺Older age (poor sphincter)
🔺Abdominal obesity
🔺Fertility preservation
Options 👇🏽

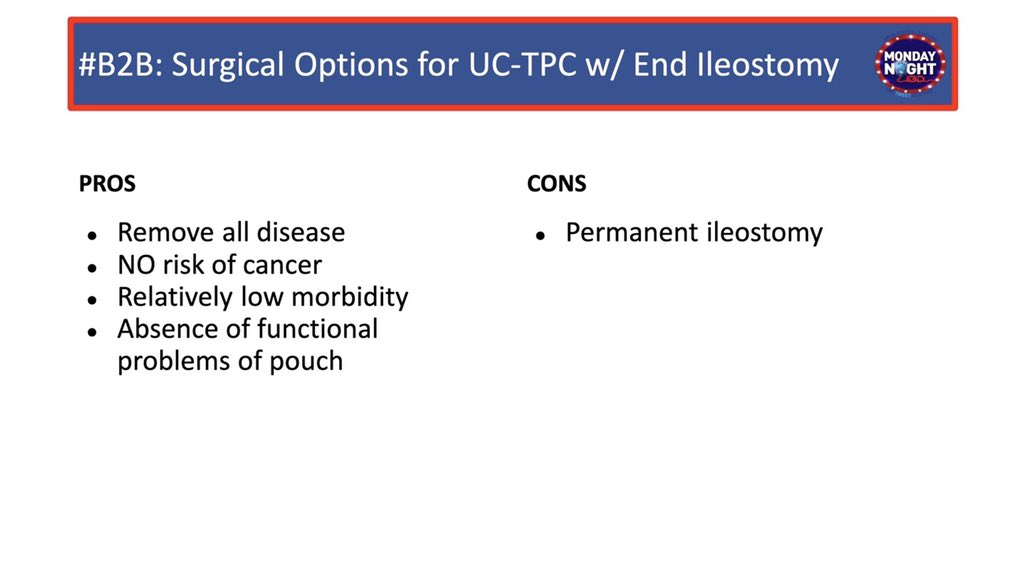
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 12/ TPC with Brooke ileostomy:
🔺Move end of SB out through opening in abd wall (stoma)
🔺Allows waste 💩 to exit body
🔺External bag worn over opening for waste
🏁Brooke ileostomies are incontinent = stool flows in bag freely
🔺Move end of SB out through opening in abd wall (stoma)
🔺Allows waste 💩 to exit body
🔺External bag worn over opening for waste
🏁Brooke ileostomies are incontinent = stool flows in bag freely

@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 13/ TPC w/Kock pouch:
🔺Internal ileal pouch+nipple valve+ileal conduit leading to cutaneous stoma
🔺Koch pouch is a continent ostomy
🚫external bag
🔺Pt inserts thin catheter into stoma to empty reservoir into 🚽 🏁least common b/c of complications (eg slippage of nipple valve)
🔺Internal ileal pouch+nipple valve+ileal conduit leading to cutaneous stoma
🔺Koch pouch is a continent ostomy
🚫external bag
🔺Pt inserts thin catheter into stoma to empty reservoir into 🚽 🏁least common b/c of complications (eg slippage of nipple valve)

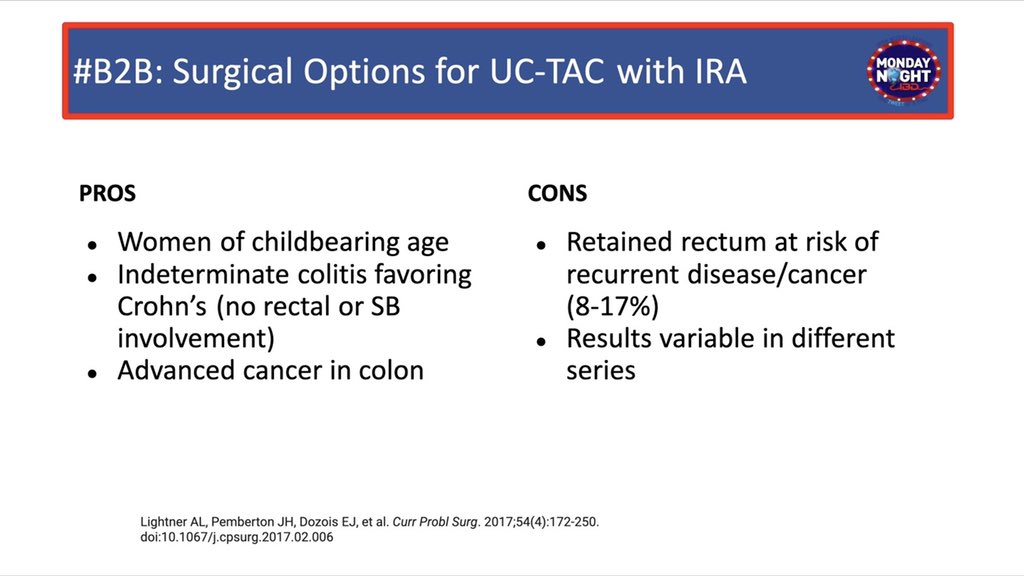
@MondayNightIBD @SobiaMujtabaMD @FezaRemziMD @DCharabaty 14/ TAC with ileorectal anastomosis (IRA)
〽In select patients, rare to have disease-free rectum
〽️Avoids pelvic dissection→ ↓risk of infertility or sexual dysfunction
🏁Option in M/F of childbearing age
〽In select patients, rare to have disease-free rectum
〽️Avoids pelvic dissection→ ↓risk of infertility or sexual dysfunction
🏁Option in M/F of childbearing age
• • •
Missing some Tweet in this thread? You can try to
force a refresh