#Tweetorial on #ASNC2020 session
⚡Selecting Between Different Functional Tests⚡
☢ vs 🧲 vs ⏺ ❓
🔘 Strengths/Limits of Lesion Specific vs Myocardial Ischemia
🔘 Comparing Dx Accuracy of Tests
🔘 Ischemia Testing in #INOCA
🔘 How to Select Best Noninvasive Test
1/9
⚡Selecting Between Different Functional Tests⚡
☢ vs 🧲 vs ⏺ ❓
🔘 Strengths/Limits of Lesion Specific vs Myocardial Ischemia
🔘 Comparing Dx Accuracy of Tests
🔘 Ischemia Testing in #INOCA
🔘 How to Select Best Noninvasive Test
1/9
https://twitter.com/coronarydoc/status/1309649449162092544
#ASNC2020 #cvNuc
2/9
Dr Di Carli
☢ Issues with proposed #FFR threshold 0.8
☢ Exercise MPI correlates well with FFR but not at 0.8
☢ Benefit of FFR-guided revasc dominantly occurs w/ thresholds <0.8
☢ Quantification of lesion-specific #ischemia insufficient for patient mgmt
2/9
Dr Di Carli
☢ Issues with proposed #FFR threshold 0.8
☢ Exercise MPI correlates well with FFR but not at 0.8
☢ Benefit of FFR-guided revasc dominantly occurs w/ thresholds <0.8
☢ Quantification of lesion-specific #ischemia insufficient for patient mgmt




#ASNC2020 #cvNuc
3/9
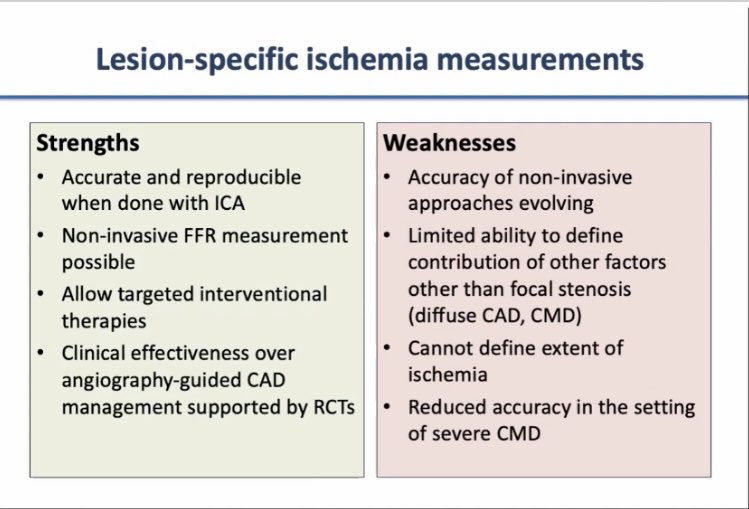
Dr Di Carli
Lesion-specific #ischemia measurements (FFR/#FFRCT)
☢ Strength
Validated against ETT/MPI
Strong outcome data
Guidelines supported
☢ Limit
Controversial threshold (0.80 vs MPI-validated 0.66)
⬆ microvasc resist causes FFR pseudonormalization
3/9
Dr Di Carli
Lesion-specific #ischemia measurements (FFR/#FFRCT)
☢ Strength
Validated against ETT/MPI
Strong outcome data
Guidelines supported
☢ Limit
Controversial threshold (0.80 vs MPI-validated 0.66)
⬆ microvasc resist causes FFR pseudonormalization


#ASNC2020 #cvNuc
4/9
Dr Di Carli
Myocardial-specific #ischemia measurements
☢ Strength
High prognostic value
Widely available
☢ Limit
Moderate accuracy w/o flow measurement
Affected by more factors than epicardial stenosis
4/9
Dr Di Carli
Myocardial-specific #ischemia measurements
☢ Strength
High prognostic value
Widely available
☢ Limit
Moderate accuracy w/o flow measurement
Affected by more factors than epicardial stenosis




#ASNC2020 #cvNuc
5/9
Dr Knaapen
⚡️ FFR-CT is best of both worlds:
plaque burden + stenosis severity
☢ FFR guided revasc reduces revasc & QoL but doesn’t significantly reduce MI/death
☢ Not every CT can be analyzed for FFR-CT
☢ PACIFIC: FFR-CT outperformed other modalities
5/9
Dr Knaapen
⚡️ FFR-CT is best of both worlds:
plaque burden + stenosis severity
☢ FFR guided revasc reduces revasc & QoL but doesn’t significantly reduce MI/death
☢ Not every CT can be analyzed for FFR-CT
☢ PACIFIC: FFR-CT outperformed other modalities




#ASNC2020 #cvNuc
6/9
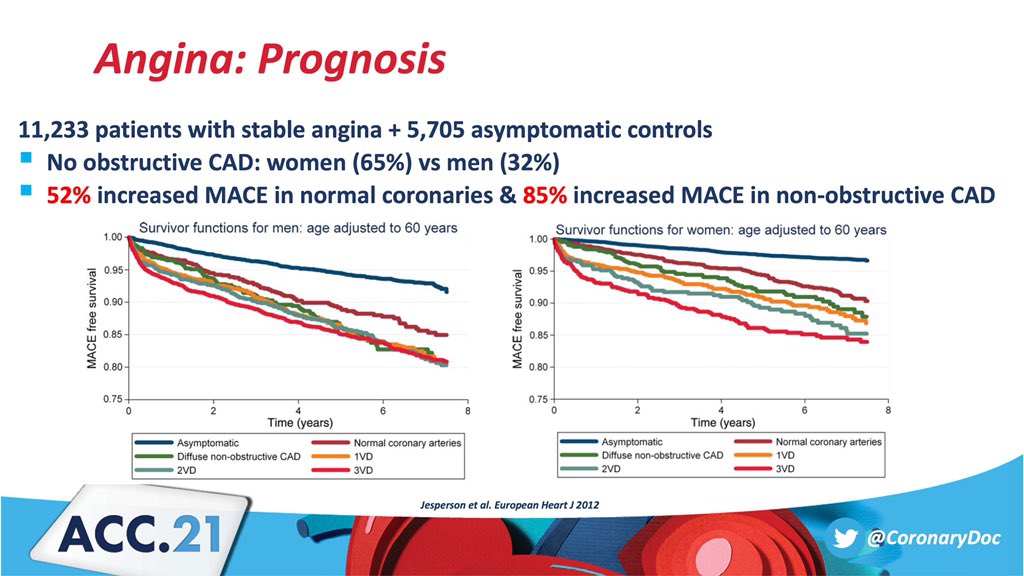
Dr Taqueti @VTaqMD
☢ Large portion of pts with angina have no evidence of obstructive #CAD on anatomical testing
☢ Traditional perfusion imaging does not identify pts with #CMD
☢ #CMD (#CFR<2.0) present in ~50% of pts with angina
6/9
Dr Taqueti @VTaqMD
☢ Large portion of pts with angina have no evidence of obstructive #CAD on anatomical testing
☢ Traditional perfusion imaging does not identify pts with #CMD
☢ #CMD (#CFR<2.0) present in ~50% of pts with angina




#ASNC2020 #cvNuc @InocaInternati1
7/9
Dr Taqueti @VTaqMD
☢ #CFR is more prognostic in♀than ♂
☢ CFR is a better prognostic factor than traditional img abnormalities
☢ #thinkPET is gold standard for eval of #CMD
☢ #whyCMR can be complementary to PET specially in #MINOCA
7/9
Dr Taqueti @VTaqMD
☢ #CFR is more prognostic in♀than ♂
☢ CFR is a better prognostic factor than traditional img abnormalities
☢ #thinkPET is gold standard for eval of #CMD
☢ #whyCMR can be complementary to PET specially in #MINOCA




#ASNC2020 #cvNuc
8/9
Dr Berman
How to select?
• Dx
• Guiding mgmt (survival benefit & Sx)
☢ Knowing plaque burden beyond lumen is important b/c quantitative plaque assessment predicts outcome
☢ #CFR is important b/c FFR does not assess diffuse atherosclerosis, #CMD #INOCA
8/9
Dr Berman
How to select?
• Dx
• Guiding mgmt (survival benefit & Sx)
☢ Knowing plaque burden beyond lumen is important b/c quantitative plaque assessment predicts outcome
☢ #CFR is important b/c FFR does not assess diffuse atherosclerosis, #CMD #INOCA




#ASNC2020 #cvNuc
9/9
Dr Berman
☢ In PACIFIC intention to Dx, PET was superior (17% could not have FFRCT)
☢ Dx of #INOCA needs presence of ischemia & absence of obst CAD
☢ If interested in knowing CAD, knowledge of coronary anatomy (stenosis, plaque burden/type) is critical
9/9
Dr Berman
☢ In PACIFIC intention to Dx, PET was superior (17% could not have FFRCT)
☢ Dx of #INOCA needs presence of ischemia & absence of obst CAD
☢ If interested in knowing CAD, knowledge of coronary anatomy (stenosis, plaque burden/type) is critical




@venkmurthy @Allison_Dupont @mhammadah @ozlembilen2 @Bob_the_PA @Arzanauskaite @PanithayaC @a_l_bailey @MinnowWalsh @DrSheilaSahni @DocSavageTJU @DavidWienerMD @EGarciaSayan @JGrapsa @heartdocandcrew @Piotr_JSlomka @fischman_david @lamelaspablo @Pooh_Velagapudi @DrToniyaSingh
A Bonus Summary Slide from Dr Berman @danielbermanmd
⚡Selecting Between Different Functional Tests⚡
#Tweetorial #ASNC2020 #thinkPET #cvNuc #yesCCT #whyCMR #CardioTwitter #INOCA #MINOCA #ACCImaging
@MyASNC @Heart_SCCT @SCMRorg @venkmurthy @DavidLBrownMD @InocaInternati1
⚡Selecting Between Different Functional Tests⚡
#Tweetorial #ASNC2020 #thinkPET #cvNuc #yesCCT #whyCMR #CardioTwitter #INOCA #MINOCA #ACCImaging
@MyASNC @Heart_SCCT @SCMRorg @venkmurthy @DavidLBrownMD @InocaInternati1

• • •
Missing some Tweet in this thread? You can try to
force a refresh