1/@HoustonAETC lunch & learns are 🔥!
@MelanieGoebelMD gave a fantastic talk on primary manifestations of skin diseases in PWH (people with HIV)
Let's review rapid-fire style...
#IDFellows #IDTwitter #DermTwitter #MedTwitter @idfellows @MedTweetorials
@MelanieGoebelMD gave a fantastic talk on primary manifestations of skin diseases in PWH (people with HIV)
Let's review rapid-fire style...
#IDFellows #IDTwitter #DermTwitter #MedTwitter @idfellows @MedTweetorials
https://twitter.com/HoustonAETC/status/1303742056511279118
2/
30YOM with well-controlled HIV and several months of this itchy red rash with silvery scales:
30YOM with well-controlled HIV and several months of this itchy red rash with silvery scales:

3/What is the most likely diagnosis?
4/Answer: Psoriasis
🔸Overall prevalence in PWH ≈ non-PWH
🔸But PWH have ⬆️ psoriatic arthritis, inverse psoriasis (axilla, intertriginous areas), and severe psoriasis
🔸Tx: ART, topical steroids, systemic treatment (methotrexate)
🔸Overall prevalence in PWH ≈ non-PWH
🔸But PWH have ⬆️ psoriatic arthritis, inverse psoriasis (axilla, intertriginous areas), and severe psoriasis
🔸Tx: ART, topical steroids, systemic treatment (methotrexate)
5/
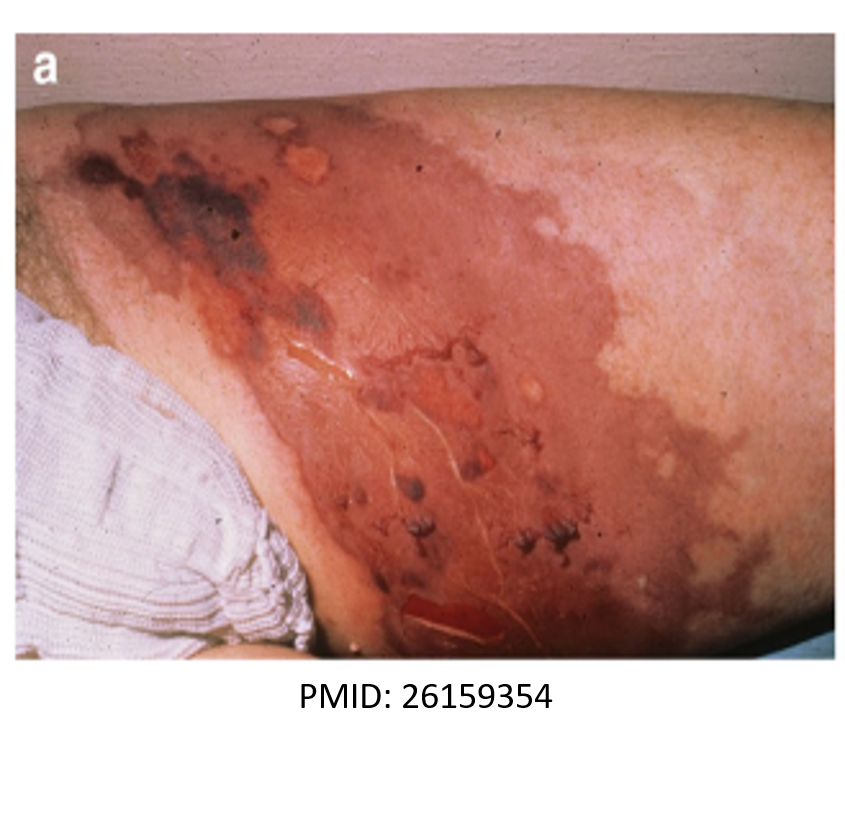
60YOM with unsheltered homelessness, HIV (CD4=7). He developed several months of this intensely pruritic skin eruption involving the "V" area of his chest, dorsal forearms, and face. He is not on any medications.
60YOM with unsheltered homelessness, HIV (CD4=7). He developed several months of this intensely pruritic skin eruption involving the "V" area of his chest, dorsal forearms, and face. He is not on any medications.

6/What is the most likely diagnosis?
7/Answer: Photodermatitis (darkening of skin exposed to sun)
🔸5% of PWH, CD4 <200, 6x more likely in AA
🔸HIV is photosensitizing➡️dysfunctional free radical scavenging pathways
🔸⬆️risk w TMP-SMX, NSAIDS, some ART
🔸Tx: ART, sun protection, topical steroids
🔸5% of PWH, CD4 <200, 6x more likely in AA
🔸HIV is photosensitizing➡️dysfunctional free radical scavenging pathways
🔸⬆️risk w TMP-SMX, NSAIDS, some ART
🔸Tx: ART, sun protection, topical steroids

8/
26YOM with HIV (CD4=22) developed these nodular itchy lesions on his face, trunk, and limbs over 2 months:
26YOM with HIV (CD4=22) developed these nodular itchy lesions on his face, trunk, and limbs over 2 months:

9/What is the most likely diagnosis?
10/Answer: Prurigo nodularis
🔸Associated with other systemic diseases👉DM, CKD, CVD, HCV
🔸⬆️ frequency if CD4 < 50
🔸Pathogenesis unknown, ⁉️ Th2 cytokines
🔸Tx: ART, topical steroids, antihistamines, emollients, phototherapy, thalidomide (refractory PN)
🔸Associated with other systemic diseases👉DM, CKD, CVD, HCV
🔸⬆️ frequency if CD4 < 50
🔸Pathogenesis unknown, ⁉️ Th2 cytokines
🔸Tx: ART, topical steroids, antihistamines, emollients, phototherapy, thalidomide (refractory PN)
11/
20YO developed severe generalized itching and multiple discrete papules over her face, trunk, arms, and the dorsum of her hands over 4 months. HIV test was positive.
20YO developed severe generalized itching and multiple discrete papules over her face, trunk, arms, and the dorsum of her hands over 4 months. HIV test was positive.

12/What is the most likely diagnosis?
13/Answer: Papular pruritic eruption
🔸Pruritic, skin-colored papules, +/- post-inflammatory hyperpigmentation
🔸Common in sub-Saharan Africa, tropics
🔸Pathophys: bug bites hypersensitivity
🔸⬇ CD4 ⬆️severity of eruption
🔸Tx: ART, antihistamines, topical steroids
🔸Pruritic, skin-colored papules, +/- post-inflammatory hyperpigmentation
🔸Common in sub-Saharan Africa, tropics
🔸Pathophys: bug bites hypersensitivity
🔸⬇ CD4 ⬆️severity of eruption
🔸Tx: ART, antihistamines, topical steroids
14/
22YOM with HIV on ART has this recurrent dry pruritic rash in his right elbow flexure:
22YOM with HIV on ART has this recurrent dry pruritic rash in his right elbow flexure:

15/What is the most likely diagnosis?
16/Answer: Atopic dermatitis
🔸Seen in 30-50% of PWH
🔸Common in those with CD4 nadir < 200
🔸Pathogenesis: hypereosinophilia, high levels of IgE secondary to Th1-Th2 imbalance
🔸Rx: topical steroids, antihistamines
🔸Recurs even with appropriate ART
🔸Seen in 30-50% of PWH
🔸Common in those with CD4 nadir < 200
🔸Pathogenesis: hypereosinophilia, high levels of IgE secondary to Th1-Th2 imbalance
🔸Rx: topical steroids, antihistamines
🔸Recurs even with appropriate ART
17/
38YOF with worsening itchy scaly patches on her arms and legs over several years. She recently tested positive for HIV (CD4=37).
38YOF with worsening itchy scaly patches on her arms and legs over several years. She recently tested positive for HIV (CD4=37).

18/What is the most likely diagnosis?
19/Answer: Xerosis (severe dry skin)
🔸Very common (20% in PWH)
🔸Severity correlates with declining CD4
🔸Pathogenesis: changes in microcirculation, decreased skin innervation, altered mast cell population in skin
🔸Tx: ART, emollients, antihistamines
🔸Very common (20% in PWH)
🔸Severity correlates with declining CD4
🔸Pathogenesis: changes in microcirculation, decreased skin innervation, altered mast cell population in skin
🔸Tx: ART, emollients, antihistamines
20/
42YOM with HIV started ART 3 months ago. He recently developed this intensely itchy follicular papular eruption involving his face, chest, and back:
42YOM with HIV started ART 3 months ago. He recently developed this intensely itchy follicular papular eruption involving his face, chest, and back:

21/What is the most likely diagnosis?
22/Answer: Eosinophilic folliculitis
🔸⬆️risk if CD4<250
🔸Can present as IRIS
🔸Pathogenesis: ⬆️IL-4 and IL-5 👉Peripheral eosinophilia, elevated IgE in 25-50%
🔸Tx: ART, topical steroids, phototherapy, itraconazole
🔸⬆️risk if CD4<250
🔸Can present as IRIS
🔸Pathogenesis: ⬆️IL-4 and IL-5 👉Peripheral eosinophilia, elevated IgE in 25-50%
🔸Tx: ART, topical steroids, phototherapy, itraconazole
23/
No clues for this one. Picture = 1000 words.
No clues for this one. Picture = 1000 words.

24/What is the most likely diagnosis?
25/Answer: seborrheic dermatitis
🔸Inflammation of sebaceous glands 👉erythema, scaling of central face, nasolabial folds, scalp
🔸Seen in up to 80% of PWH 👉worse w/ ⬇️CD4
🔸Pathogenesis: ? Hypersensitivity to fungus
🔸Tx: topical antifungals, oral itraconazole if severe
🔸Inflammation of sebaceous glands 👉erythema, scaling of central face, nasolabial folds, scalp
🔸Seen in up to 80% of PWH 👉worse w/ ⬇️CD4
🔸Pathogenesis: ? Hypersensitivity to fungus
🔸Tx: topical antifungals, oral itraconazole if severe
26/Today, we covered the primary manifestations of skin diseases in HIV.
Stay tuned for part 2 in the upcoming weeks!
Stay tuned for part 2 in the upcoming weeks!

27/Additional references:
pubmed.ncbi.nlm.nih.gov/21261982/
pubmed.ncbi.nlm.nih.gov/16377853/
iasusa.org/dermatologic-m…
pubmed.ncbi.nlm.nih.gov/21261982/
pubmed.ncbi.nlm.nih.gov/16377853/
iasusa.org/dermatologic-m…
• • •
Missing some Tweet in this thread? You can try to
force a refresh