The Barrington Declaration from the quadrangles of Yale, Stanford + Oxford: "People who are more at risk may participate if they wish, while society as a whole enjoys the protection conferred upon the vulnerable by those who have built up herd immunity." (1) Er....No. 

How long does immunity last?
Will herd immunity be achieved?
What about Long Covid?
Sweden tried this with 582 deaths/million, Norway 51 deaths/million didn't.
How practical is shielding 30% of the population? No data.
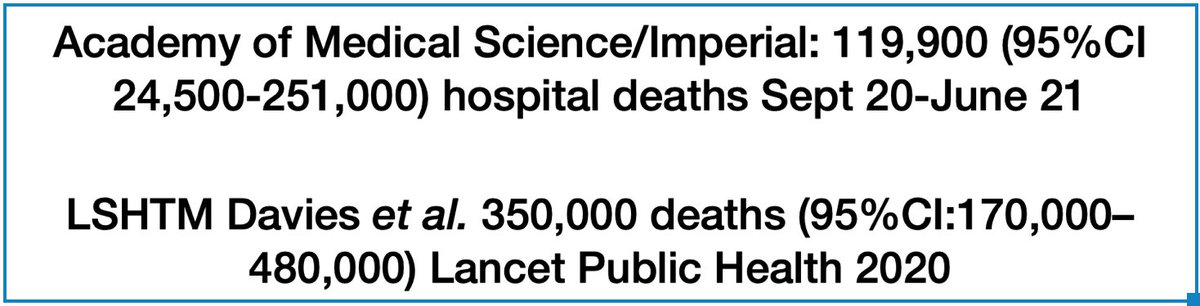
What are their death projections v economic benefits?
(2)
Will herd immunity be achieved?
What about Long Covid?
Sweden tried this with 582 deaths/million, Norway 51 deaths/million didn't.
How practical is shielding 30% of the population? No data.
What are their death projections v economic benefits?
(2)
It seems odd that the countries who failed to tackle the pandemic effectively, which the Barrington people want, suffered the biggest economic hit. (3)

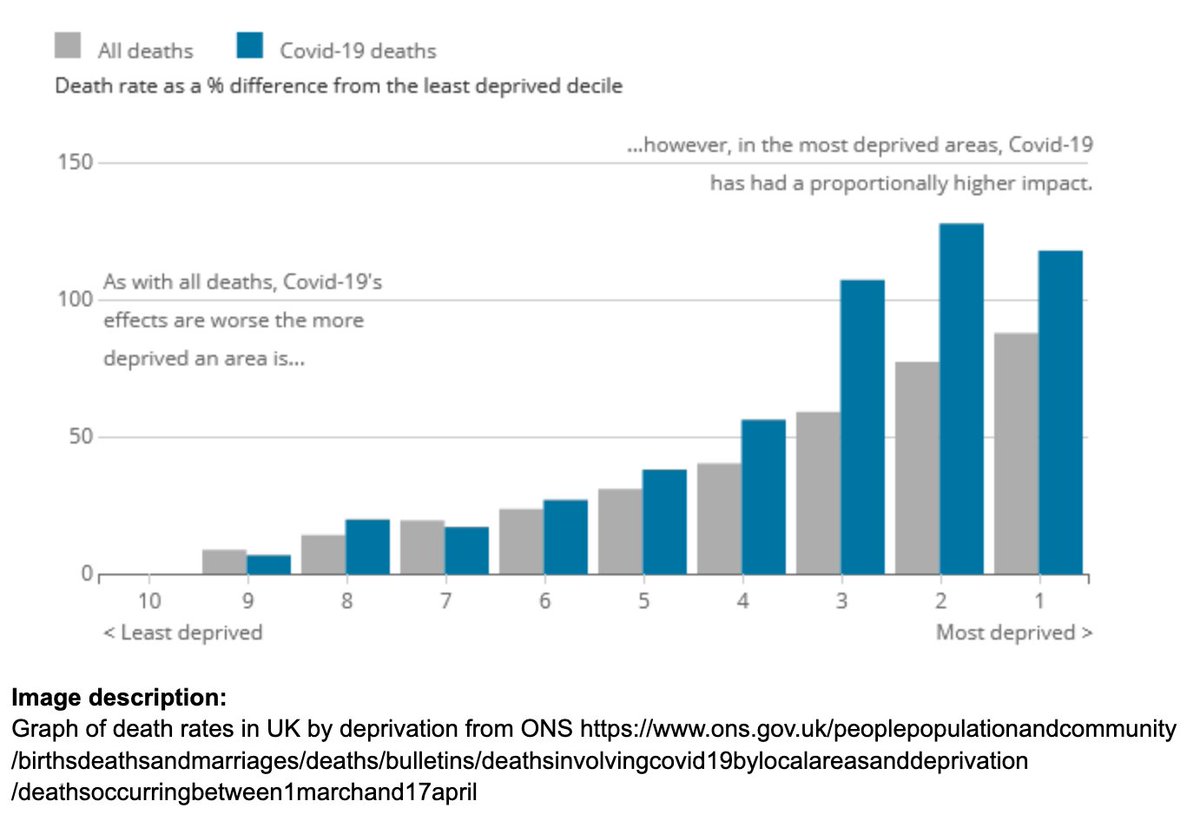
And what about the awful and unequal casualty rates in the poorest, BME and frontline worker groups who will suffer the consequences of a reckless, untested policy to 'take it on the chin'? (4)
Read Independent SAGE report why this is wrong. Independent SAGE report – independentsage.org/a-deliberate-p… (5)
Also see the Science Media response from other distinguished scientists and medics. sciencemediacentre.org/expert-reactio… (6)
Interesting also that Professor Carl Heneghan didn't sign it. @carlheneghan (7)
• • •
Missing some Tweet in this thread? You can try to
force a refresh