I don't usually do these kinds of posts, and I hope that everyone understands my intentions are good here.
But.
In a data deficient landscape like that of #longcovid, one bad data study can create narratives that persist long after new, good data is created. I want to talk 1/
But.
In a data deficient landscape like that of #longcovid, one bad data study can create narratives that persist long after new, good data is created. I want to talk 1/
about one of these.
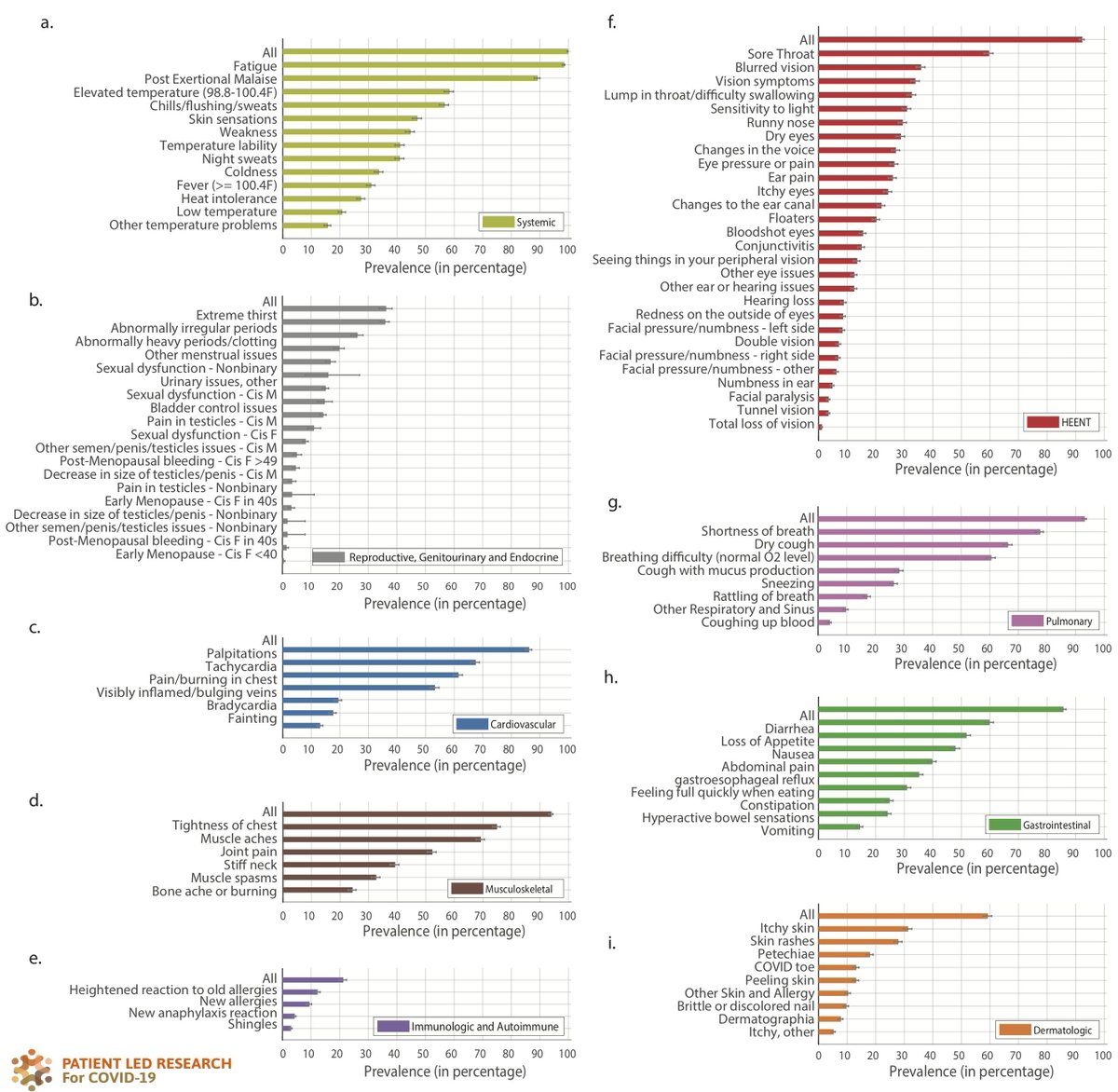
The Kings College symptom tracker is an app. Because they track symptoms over time, it gets a lot of citations on Long Covid prevalence, and also symptom prevalence.
But there are 2 *huge* issues with it:
2/
The Kings College symptom tracker is an app. Because they track symptoms over time, it gets a lot of citations on Long Covid prevalence, and also symptom prevalence.
But there are 2 *huge* issues with it:
2/
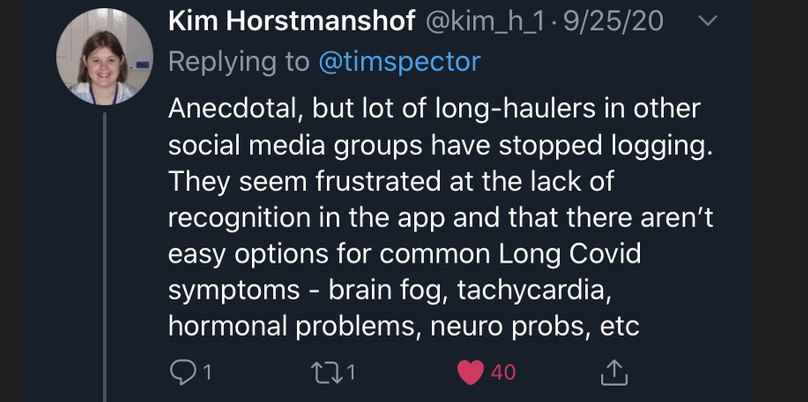
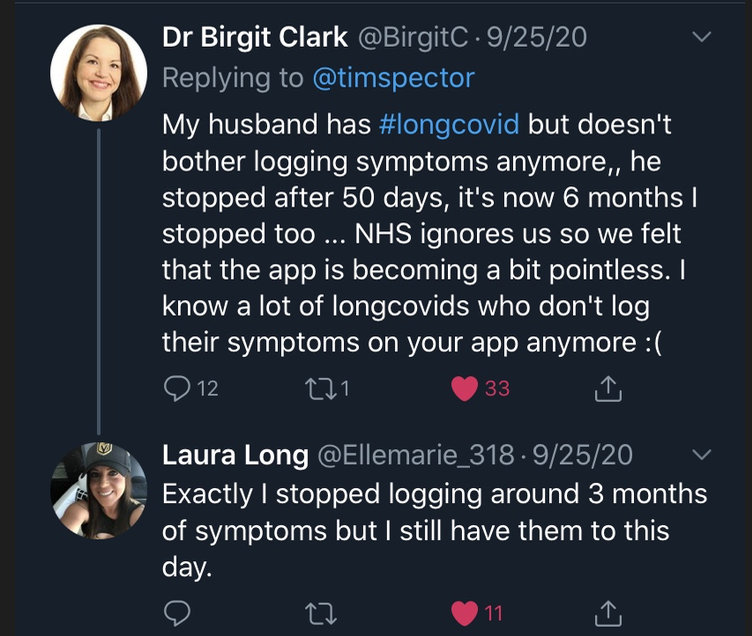
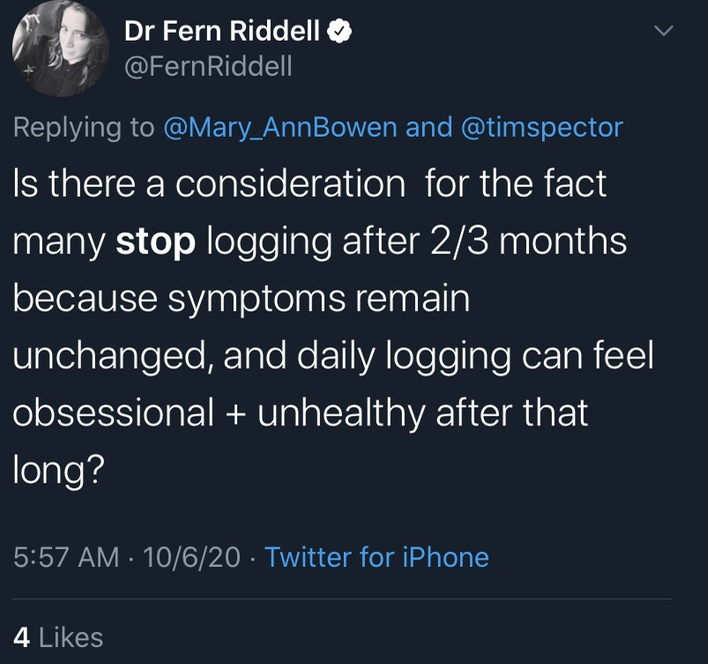
1) Because it's an app, it gets exhausting to use, and people stop using it. This is a known and public problem, understood by Tim himself:
3/
3/

There are so many reasons people stop using it
4/
4/

More
5/
5/
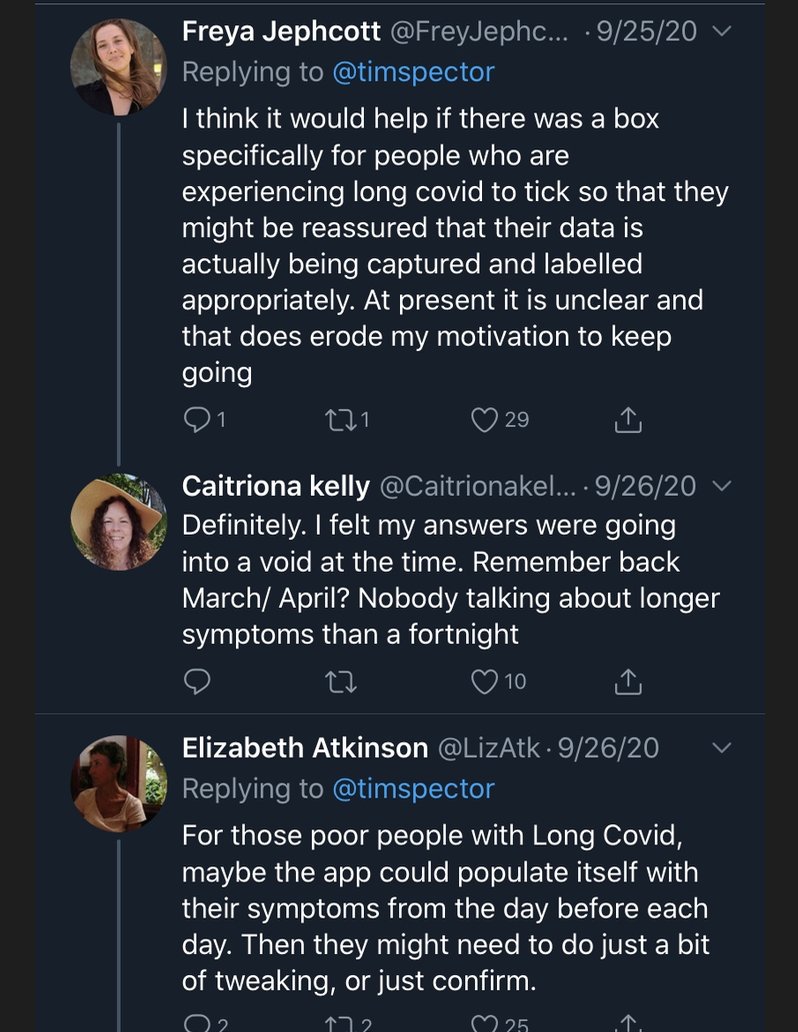
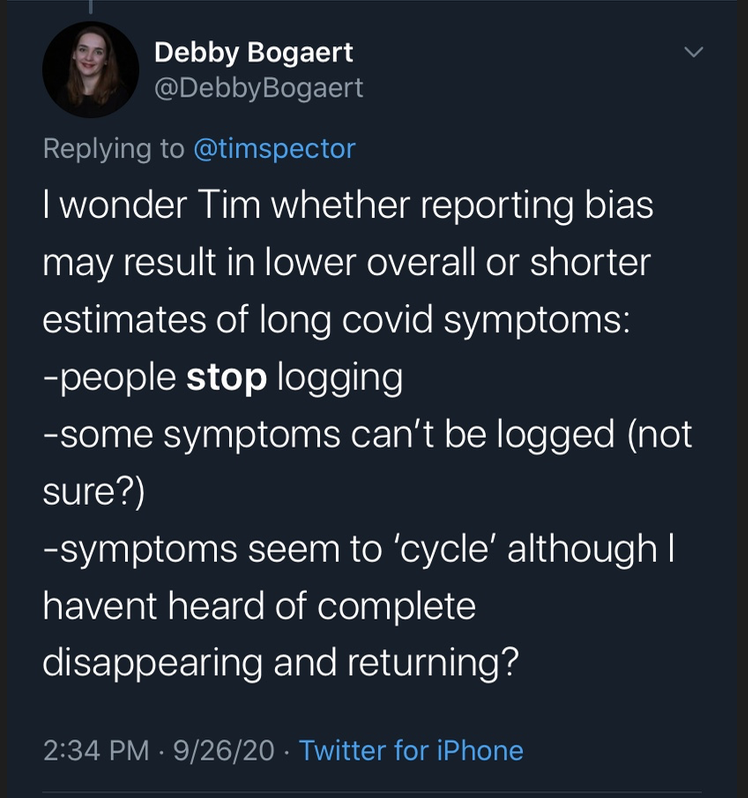
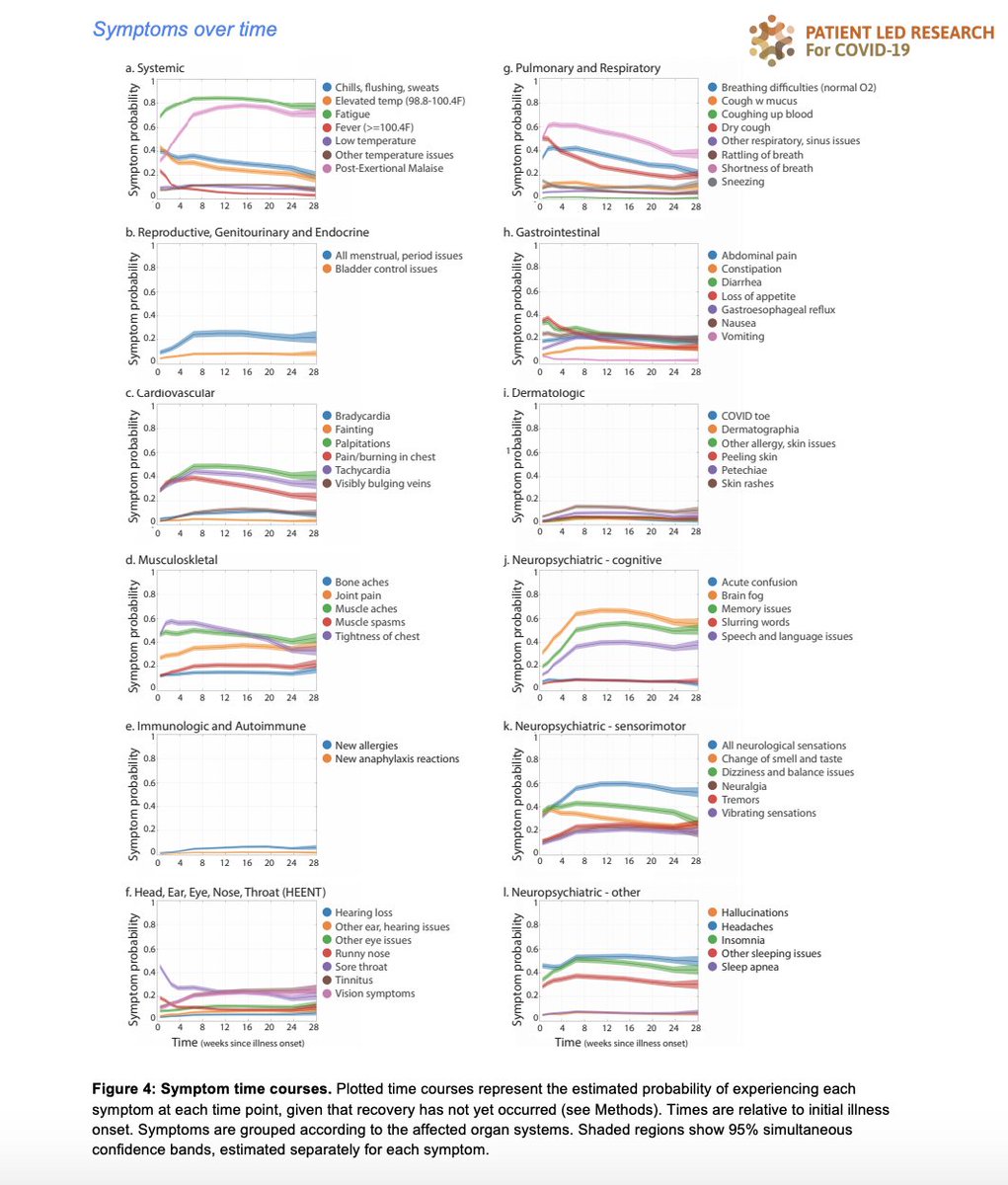
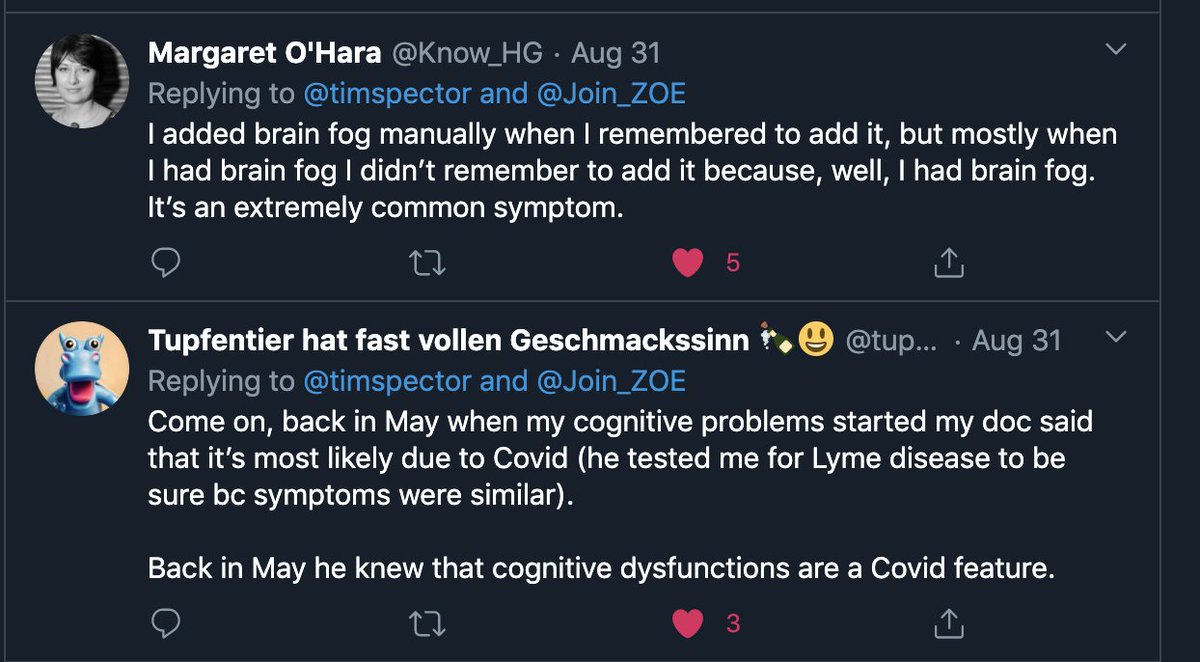
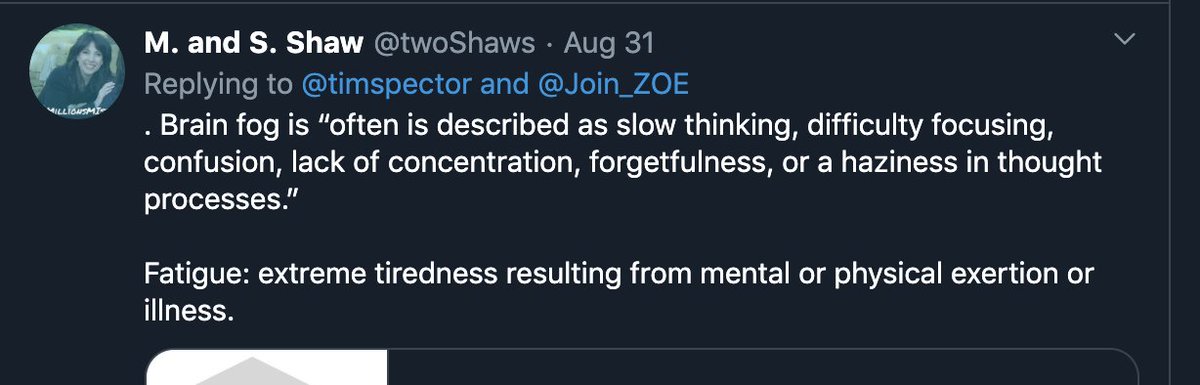
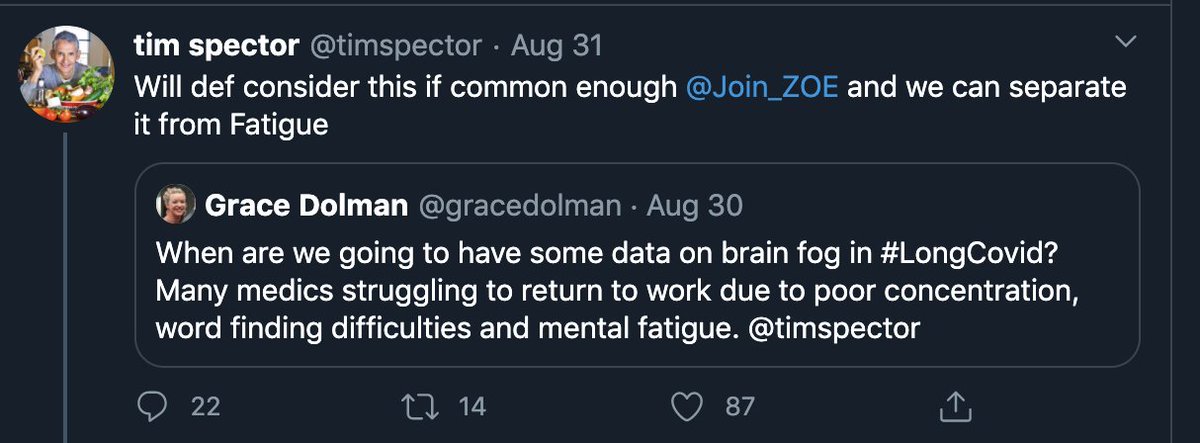
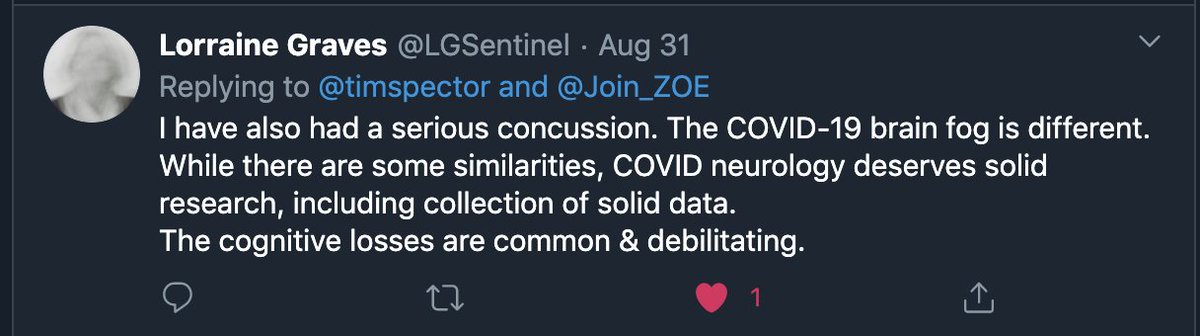
2) The other big issue is that the app didn't (possibly still doesn't) collect data on one of the most prevalent symptoms - "brain fog"/cognitive dysfunction - despite requests from patients to do so - despite neurological symptoms generally lasting longer:
6/
6/
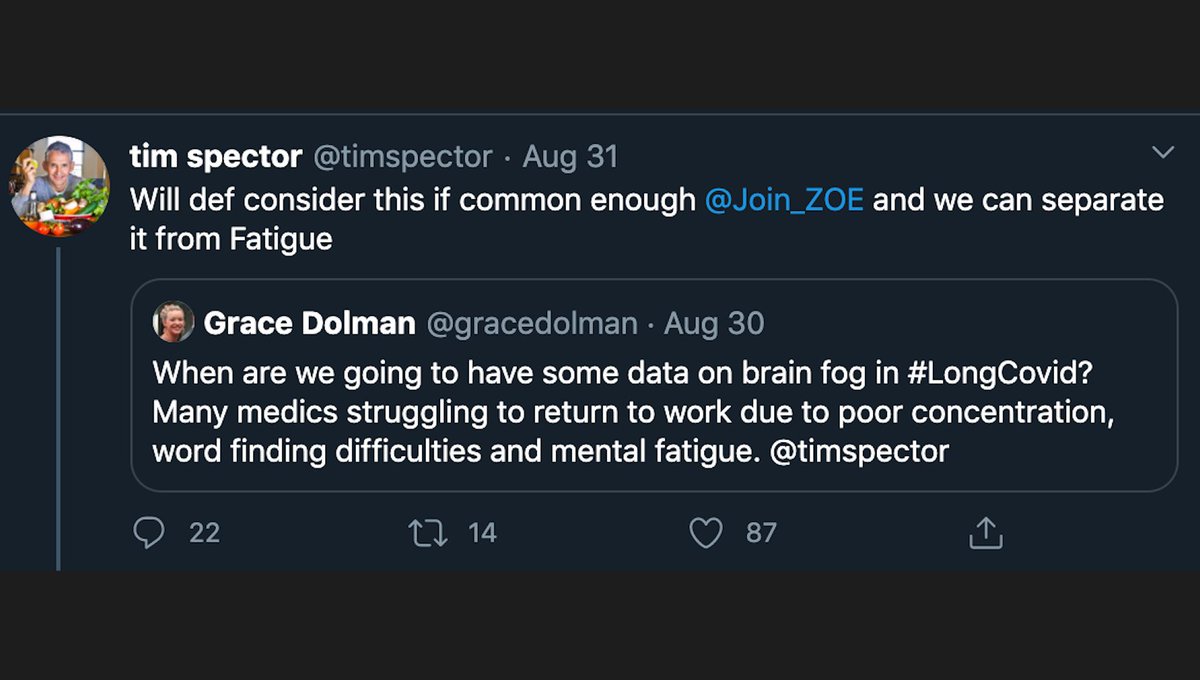
Again, so many requests from patients:
7/
7/

8/

Tim Spector/team publish those numbers as Long Covid prevalence anyway, & claim that just 1.5% of COVID patients are still symptomatic at 3 months🙃
institute.global/policy/long-co…
There are few official population studies (which is part of the problem)-let's look at what they say:
9/
institute.global/policy/long-co…
There are few official population studies (which is part of the problem)-let's look at what they say:
9/
CDC's report says that 35% are not recovered at 3 weeks cdc.gov/mmwr/volumes/6…
Report from Wuhan has 11.1% unrecovered at 3 months onlinelibrary.wiley.com/doi/full/10.10…
docs.google.com/spreadsheets/d…
None come close to 1.5% at 3 months - it's an order of magnitude smaller than other estimates. 10/
Report from Wuhan has 11.1% unrecovered at 3 months onlinelibrary.wiley.com/doi/full/10.10…
docs.google.com/spreadsheets/d…
None come close to 1.5% at 3 months - it's an order of magnitude smaller than other estimates. 10/
And the fact is, you can't put numbers out into the world without explaining the serious biases behind them and then say "take this with a grain of salt." It's been 2 days and these figures have already ended up in the BBC (bbc.com/news/health-54…) 11/

and articles like this one, with King's College team members claiming ""This is absolutely the message we should give: a small proportion have symptoms at 13 weeks, but really pretty much everybody is better by then," Dr Williams said." telegraph.co.uk/global-health/… 12/
These numbers and subsequent narratives are going to be so hard to beat, and they are going to ultimately *HARM* #longcovid patients. As the saying goes "The amount of energy needed to refute bullshit is an order of magnitude bigger than to produce it." 13/
I think Tim Spector is a good person. I'm a huge microbiome nerd and his work there is cool. But this is irresponsible, embarrassing, and needs to be in the public #longcovid awareness, if not corrected completely.
End rant.
14/
End rant.
14/
We need an acknowledgment from @KingsCollegeLon @Join_ZOE @timspector on this, and to hear clear feedback on how they are going to change going forward - including how they are going to present their numbers in public. #longcovid care depends on it.
cc @AndyChanMD @MGH_RI
15/
cc @AndyChanMD @MGH_RI
15/
The @Join_ZOE app has now paired with a millionaire's underwear company, so on top of blatantly misrepresenting the most important data (#longcovid prevalence), it's also using patients' #longcovid data for commercial partnerships.
16/
https://twitter.com/Know_HG/status/1317438243818901504
16/
What does the ZOE COVID Symptom Tracker app do with the #LongCovid patients who stop using the app?
If the patient had less than *5* symptoms on the last day they used the app, it counts them as *RECOVERED* & considers the disease ended 🙃
17/
If the patient had less than *5* symptoms on the last day they used the app, it counts them as *RECOVERED* & considers the disease ended 🙃
17/
The above is from their preprint directly! medrxiv.org/content/10.110…
If you're a #LongCovid patient with less than 5 symptoms, is your illness over?
18/
If you're a #LongCovid patient with less than 5 symptoms, is your illness over?
18/

• • •
Missing some Tweet in this thread? You can try to
force a refresh