
Check out ERC.edu and click on guidelines for public comment to see the latest changes and key recommendations #RESUS20
Systems save lives highlighting systemic changes we can make globally by engaging governments and linking up the chain of survival @fsemeraro1973 #RESUS20 #kidssavelives 

The biggest impact we can have is probably with dispatch and first responder CPR. Bystander engagement is fundamental. Is this the weakest link in the chain? Start young and implement in schools #systemssavelives #kidssavelives #checkcallcompress #callcompressdefibrillate
BLS updates with @olasveengen agonal breathing and seizures confuse the picture. These are not signs of life! #RESUS20 #CPR

Rescuers safety always comes first. PPE before CPR! we don’t want Covid fears to take us backwards in our advances #RESUS20 #AED #CPR AED's are safe to use even for lay rescuers @olasveengen


First poll of the day! Adrenaline is still in favour with @ERC_ALS_SEC @Ilcor_org @ERC_resus and with today’s delegates! #CPR #RESUS20

Controversial topics: adrenaline increases survival to hospital admission and discharge @TDjarv #RESUS20 Airways: whatever gets air in, use it. IV access before IO as it seems more effective. Ultrasound is good for identifying tamponade but not much else #controversial
We want your feedback! Get involved and tell us your thoughts #guidelines20 #RESUS20 @ERC_ALS_SEC @ERC_resus

Don’t take away from the things we know work and are easy: compressions, drugs etc just to spend time playing with ultrasound. The chain is still important #RESUS20
Post resus care with Prof Jerry Nolan #RESUS20 targets and considerations! Go read the new draft guidelines ERC.edu

Post resus care starts from the moment the patient gets ROSC. This could be pre hospital and not just the domain of our wonderful ICU colleagues #RESUS20
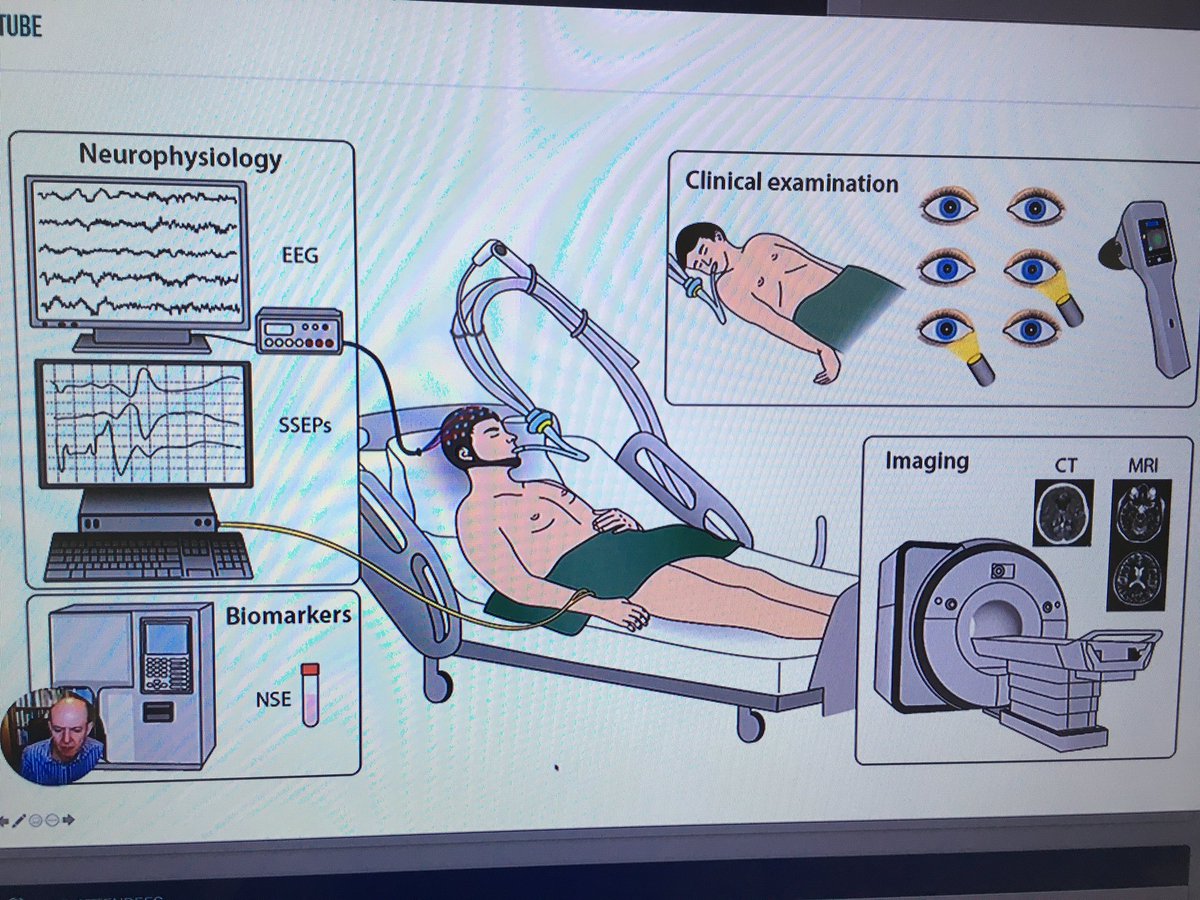
Revised prognostication algorithm #RESUS20 #postresuscare need AT LEAST 2 of these for a favourable outcome. Neuroprognostication is tricky, suggest at least 72hours but often in practice takes longer than this @ERC_ALS_SEC @ERC_resus

TTM recommendation is unchanged from 2015 guidelines. Some form of constant temp control for 32-36*c for first 72 hours. May require modifications after TTM2 #RESUS20

• • •
Missing some Tweet in this thread? You can try to
force a refresh




