Further thoughts on post-viral ME/CFS after more literature review.
Initial suspicions about infected leukocytes were too narrow.
Persistently, latently, or formerly infected cells in tissues with low turnover are a more likely culprit.
Initial suspicions about infected leukocytes were too narrow.
Persistently, latently, or formerly infected cells in tissues with low turnover are a more likely culprit.
https://twitter.com/__ice9/status/1319332569834491904
Clearance of such cells in ME/CFS patients is impaired.
https://twitter.com/__ice9/status/1319337241634873345?s=19
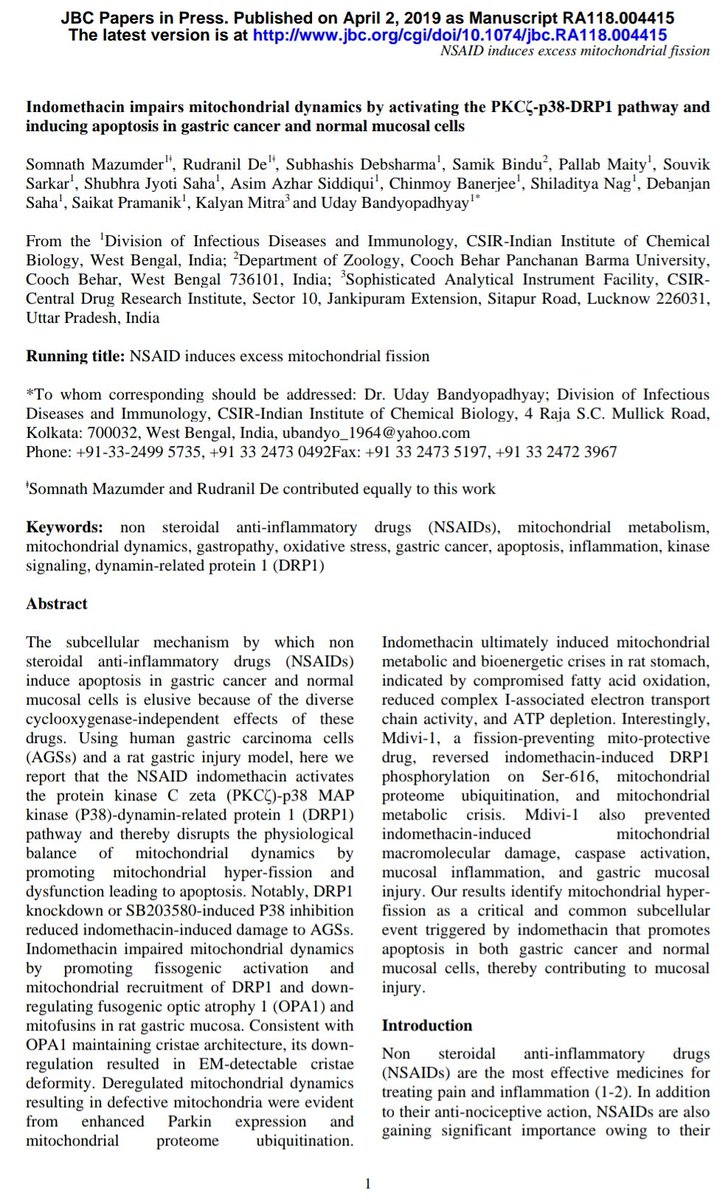
The secretome of such cells is often inflammatory (see first reference above) and has been shown to be metabolically disruptive for at least some viruses (more data on CoVs would be helpful):
https://twitter.com/__ice9/status/1319329187946205184?s=19
Some viruses, including SARS-CoV-2, are also particularly difficult to clear due to e.g. degradation and downregulation of MHC:
https://twitter.com/__ice9/status/1319343154974392321?s=19
One might expect that the lytic nature of coronaviruses would limit the importance of that issue in the long run.
But on the contrary, lingering CoV RNA and protein material (infected or surviving cells) have been detected in e.g. CNS tissue for example:
But on the contrary, lingering CoV RNA and protein material (infected or surviving cells) have been detected in e.g. CNS tissue for example:
https://twitter.com/__ice9/status/1319333789978578944?s=19
The most problematic sites for persistently, latently, or formerly infected cells producing an inflammatory or metabolically disruptive secretome should be tissues with slow turnover.
Fast: nasal, pharyngeal, mucosal, etc
Slow: alveolar, endothelial, nervous (mostly zero), etc
Fast: nasal, pharyngeal, mucosal, etc
Slow: alveolar, endothelial, nervous (mostly zero), etc



Predictions if so:
COVID-19 patients may have more fatigue after cardiopulmonary recovery if virus reached deeper into lungs, vascular endothelia, or nervous system.
Antioxidants, brief interferon/inducer use, and drugs stimulating cytotoxic lymphocyte response might help.
COVID-19 patients may have more fatigue after cardiopulmonary recovery if virus reached deeper into lungs, vascular endothelia, or nervous system.
Antioxidants, brief interferon/inducer use, and drugs stimulating cytotoxic lymphocyte response might help.
This is still somewhat speculative, study and trial data on COVID-19 patients with persistent symptoms remains limited, it is not clear how well studies on ME/CFS patients might apply to these cases, and in general the above should be viewed as preliminary.
Also POTS/dysautonomia is clearly a distinct disorder from ME/CFS, albeit often co-occurring with it.
The underlying mechanism appears to be fundamentally different, though both could be (and most likely often are) caused by viral infection.
https://twitter.com/__ice9/status/1319366027407482887?s=19
The underlying mechanism appears to be fundamentally different, though both could be (and most likely often are) caused by viral infection.
• • •
Missing some Tweet in this thread? You can try to
force a refresh