
1/13
Amazing pizza, barista level coffee, and a case involving SOB and a new pericardial effusion! Hard not to get palpitations from this amazing #CNCR by @UHCardsFellows
Episode here: cardionerds.com/72-case-report…
Here’s a brief re-cap with some of the 💯 learning
Amazing pizza, barista level coffee, and a case involving SOB and a new pericardial effusion! Hard not to get palpitations from this amazing #CNCR by @UHCardsFellows
Episode here: cardionerds.com/72-case-report…
Here’s a brief re-cap with some of the 💯 learning

2/
Mid 70s F p/w subacute onset SOB. PMHx of recurrent metastatic breast cancer s/p mastectomy, chemo/radiation. On exam, tachy, muffled heart sounds, JVD, BLE edema, and +Kussmaul's sign
Let's start with some physical exam teaching! What is Kussmaul's sign and what causes it?🤔
Mid 70s F p/w subacute onset SOB. PMHx of recurrent metastatic breast cancer s/p mastectomy, chemo/radiation. On exam, tachy, muffled heart sounds, JVD, BLE edema, and +Kussmaul's sign
Let's start with some physical exam teaching! What is Kussmaul's sign and what causes it?🤔
3/
Kussmaul's sign, when JVP doesn't ⬇️ during inspiration ➡️ poorly compliant RV d/t RV myocardium or pericardium (e.g. RV failure, RV ischemia, and occasionally Tamponade). Seen in 50% of cases of constrictive pericarditis!
Kussmaul's sign, when JVP doesn't ⬇️ during inspiration ➡️ poorly compliant RV d/t RV myocardium or pericardium (e.g. RV failure, RV ischemia, and occasionally Tamponade). Seen in 50% of cases of constrictive pericarditis!
4/
Next, TTE done showing normal EF, mod effusion, significant respirophasic tricuspid and mitral inflow variations, and R➡️L septal shift w/ inspiration.
Best clinical maneuver cinch dx of tamponade?
Next, TTE done showing normal EF, mod effusion, significant respirophasic tricuspid and mitral inflow variations, and R➡️L septal shift w/ inspiration.
Best clinical maneuver cinch dx of tamponade?
5/
Pulsus paradoxus! A⬇️SBP ≥10 is diagnostic, but a⬇️≥ 12 is 98% sens and 83% spec for tamponade. Tachy, JVP also⏫sens.
For more on using clinical signs, pulsus, and TTE to dx tamponade, see show notes!
To the cath lab🦸♂️! What might we see on RHC in tamponade?
Pulsus paradoxus! A⬇️SBP ≥10 is diagnostic, but a⬇️≥ 12 is 98% sens and 83% spec for tamponade. Tachy, JVP also⏫sens.
For more on using clinical signs, pulsus, and TTE to dx tamponade, see show notes!
To the cath lab🦸♂️! What might we see on RHC in tamponade?
6/
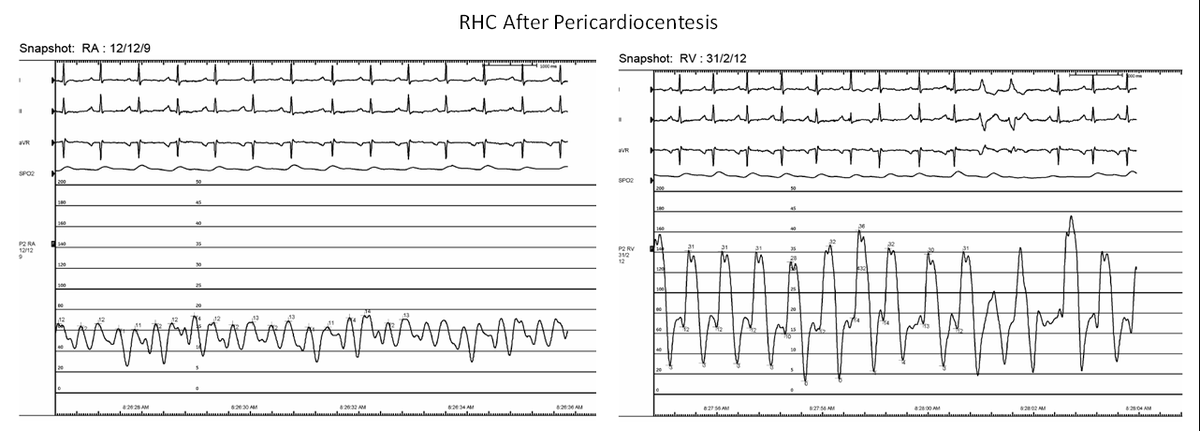
B and C, both seen in this pt!
"lose the y, you die" -@karanpdesai
Pericardiocentesis w/ 200cc bloody fluid.
Repeat RHC with improvement, but continued equalization and elevation of diastolic pressures, now with rapid y descent c/f constriction😲.
What's going on here? 🕵️♂️
B and C, both seen in this pt!
"lose the y, you die" -@karanpdesai
Pericardiocentesis w/ 200cc bloody fluid.
Repeat RHC with improvement, but continued equalization and elevation of diastolic pressures, now with rapid y descent c/f constriction😲.
What's going on here? 🕵️♂️

7/
The ever elusive effusive constrictive pericarditis (ECP)! Defined as the persistence of constrictive physiology after pericardiocentesis, it presents with S/Sx of both a clinically significant effusion AND constrictive pericarditis.
But how common is this and what causes it?
The ever elusive effusive constrictive pericarditis (ECP)! Defined as the persistence of constrictive physiology after pericardiocentesis, it presents with S/Sx of both a clinically significant effusion AND constrictive pericarditis.
But how common is this and what causes it?

8/
Risk of developing ECP related to cause of effusion
Common in TB related effusions (>50% of cases), only ~15% in effusions requiring drainage/tamponade. Even rarer in all comers with pericarditis (only 1.3%)!
Can we use TTE to identify those with effusions at risk for ECP?
Risk of developing ECP related to cause of effusion
Common in TB related effusions (>50% of cases), only ~15% in effusions requiring drainage/tamponade. Even rarer in all comers with pericarditis (only 1.3%)!
Can we use TTE to identify those with effusions at risk for ECP?

9/
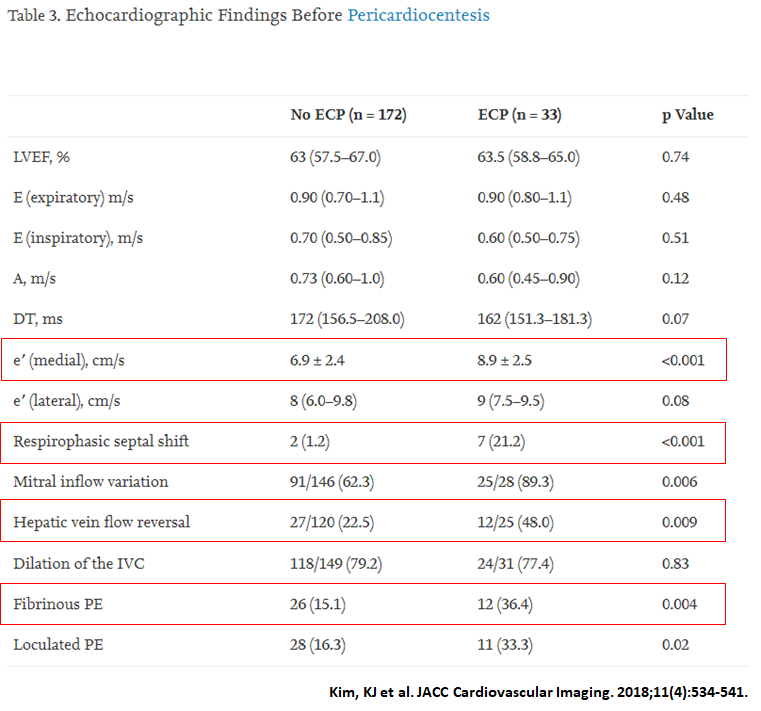
No data on TTE findings to predict ECP post drainage. More common findings in ECP:
✅⬆️Mitral medial e' velocity
✅ Respirophasic septal shift
✅ Hepatic vein flow reversal
Makes sense as these are features normally seen in CP! Post drainage TTE features also match CP
No data on TTE findings to predict ECP post drainage. More common findings in ECP:
✅⬆️Mitral medial e' velocity
✅ Respirophasic septal shift
✅ Hepatic vein flow reversal
Makes sense as these are features normally seen in CP! Post drainage TTE features also match CP

10/
For more on Dx of CP and how to differentiate it from RCM see tweetorials and show notes from:
Episode 58: cardionerds.com/58-case-report…
Tweetorial:
and
Episode 59: cardionerds.com/59-case-report…
Tweetorial:
Now how do we treat this?
For more on Dx of CP and how to differentiate it from RCM see tweetorials and show notes from:
Episode 58: cardionerds.com/58-case-report…
Tweetorial:
https://twitter.com/EvelynSongMD/status/1307343536539480065?s=20
and
Episode 59: cardionerds.com/59-case-report…
Tweetorial:
https://twitter.com/varghes_bibin/status/1309656094994845700?s=20
Now how do we treat this?


11/
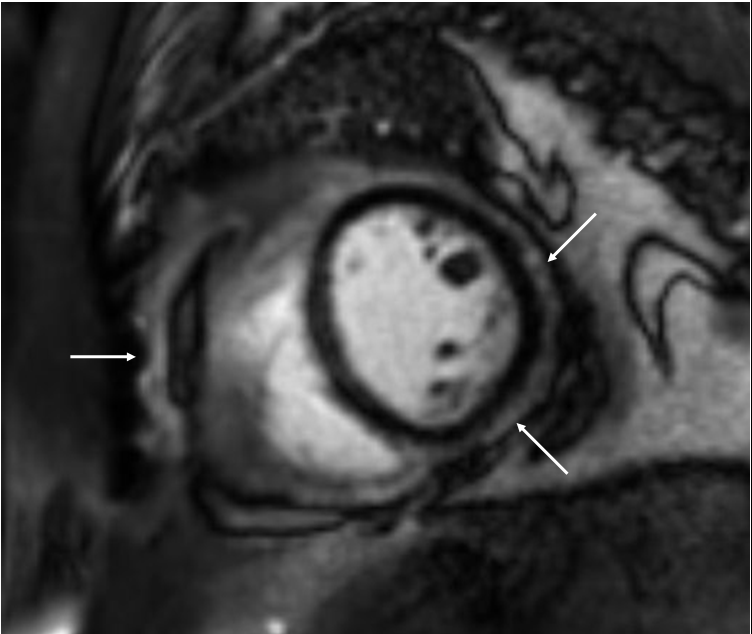
No guidelines, but a few🔑🦪:
✅Trial anti-inflammatories, esp. if evidence of pericardial 🔥 (see cMRI with LGE from our case!)
✅Pericardiocentesis might provide temp. relief
✅Pericardiectomy for refractory S/Sx, but often need to remove visceral layer (⬆️difficulty!)
No guidelines, but a few🔑🦪:
✅Trial anti-inflammatories, esp. if evidence of pericardial 🔥 (see cMRI with LGE from our case!)
✅Pericardiocentesis might provide temp. relief
✅Pericardiectomy for refractory S/Sx, but often need to remove visceral layer (⬆️difficulty!)
12/
Need for pericardiectomy also varies by etiology. Overall the majority (~65%) of patients will require pericardiectomy within the 1st year of diagnosis.
As for our patient, cytology was c/w malignancy. Ultimately underwent pericardiectomy and had an excellent response!
Need for pericardiectomy also varies by etiology. Overall the majority (~65%) of patients will require pericardiectomy within the 1st year of diagnosis.
As for our patient, cytology was c/w malignancy. Ultimately underwent pericardiectomy and had an excellent response!
13/
That’s our case! Thanks again to the amazing @UHCardsFellow @TCCardio, @HaythamMously, and Jamal Hajjari!
As always special thanks to @cardionerds and @karanpdesai for their help and constant dedication to #MedEd
Sign up for THE HEARTBEAT: eepurl.com/hazGYL
That’s our case! Thanks again to the amazing @UHCardsFellow @TCCardio, @HaythamMously, and Jamal Hajjari!
As always special thanks to @cardionerds and @karanpdesai for their help and constant dedication to #MedEd
Sign up for THE HEARTBEAT: eepurl.com/hazGYL
• • •
Missing some Tweet in this thread? You can try to
force a refresh


