
Why does chemotherapy kill cancerous but not normal cells? Most cancer biologists would answer this by stating that chemotherapy is selectively toxic to proliferating cells, and that cancer cell proliferate more than normal cells. Not exactly - there's a lot more to it.
https://twitter.com/trendscancer/status/1321125361602695168
Many normal tissues, like bone marrow and gut cells are actually more proliferative than even the most aggressive cancers. E.g. pro-myelocytes have a doubling time of around 17 hrs whilst even aggressive epithelial tumors double every 2-3 weeks or so.
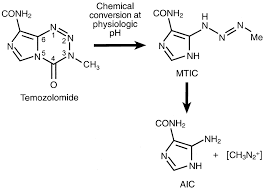
So while many chemotherpeutics (e.g. #Temozolomide for GBM) show extensive myelotoxicity as a side effect, clinically useful ones are able to kill cancerous cells more efficaciously than normal ones, even if the latter proliferate faster, like pro-myelocytes.
How do they do it?
How do they do it?
Turns out that many cytotoxic chemotherpeutics are complex pro-drugs, that one was or another, are selectively bioactivated (or inactivated) in cancer versus normal tissue. Common chemos: cyclophosphamide, #temozolomide, 5-FU, irinotecan, methotrexate, cis-platin are pro-drugs! 
One way or another, the degree of bioactivation of these pro-drugs is higher in cancerous versus normal fast proliferating tissues (we lay out the details for specific examples in the paper).
What would happen if the active, rather than pro-drug is administered directly?
What would happen if the active, rather than pro-drug is administered directly?
Massive myelotoxicity with no therapeutic window for treatment of cancer E.g. MTIC (activated for of #Temozolomide), nitrogen mustart (activated form of #Cyclophosphamide), #SN38 (active form of #irinotecan).
That normal tissues proliferate faster than most tumors has important ramifications for cancer drug development and explains why "pure" mitotic inhibitors like those targeting #AURKA, #AURKB, #PLK1, #MPS1, #CDK1, and DNA polymerase, have remained stalled in phase I trials.
Accross the board, inhibitors of mitotic kinases (like AURKA etc) have led to massive neutropenia, precluding advancement beyond phase I/II.
In this opinion piece, we lay out how this otherwise discarded family of cancer drugs could be resurected, taking cues from the pro-drug nature of cytoxic chemotherapeutics.
An illustration of this idea, though with a different approach, was recently provided by #Immunomedics's SN-38-Trop2 conjugate.
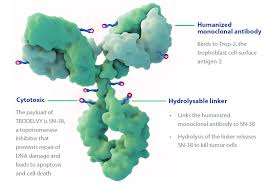
SN38 is a clean mitotic poison (Topoisomerase is expressed predominantly in proliferating cells, cancerous or normal) and its on-target activity in bone marrow cells leads to massive #neutropenia.
The re-directing or selective enrichement of SN-38 in the peri-tumoral environment by conjugation with the Trop2 antibody (labile by esterases and released peri-tumorally rather than intracellularly) vs bone marrow now allows for a therapeutic window.
Incidentally, neutropenia is still a major side effect, most likely because of release of active SN-38 by linker esterase hydrolysis. But way better than with SN-38 alone.
Our paper suggests that other mitotic kinase inhibitors could do just as well, and potentially even better, than SN-38, as conjugates of ADCs.
• • •
Missing some Tweet in this thread? You can try to
force a refresh


