A thread on knee injuries in females and strategies to help minimize their potential
Weakness of the hip abductor & external rotator (ER) muscles is surprisingly common in otherwise normal & healthy females (Malinzak et al, 2001; Robinson, 2007).
That is just one piece of the..
Weakness of the hip abductor & external rotator (ER) muscles is surprisingly common in otherwise normal & healthy females (Malinzak et al, 2001; Robinson, 2007).
That is just one piece of the..

overall puzzle.
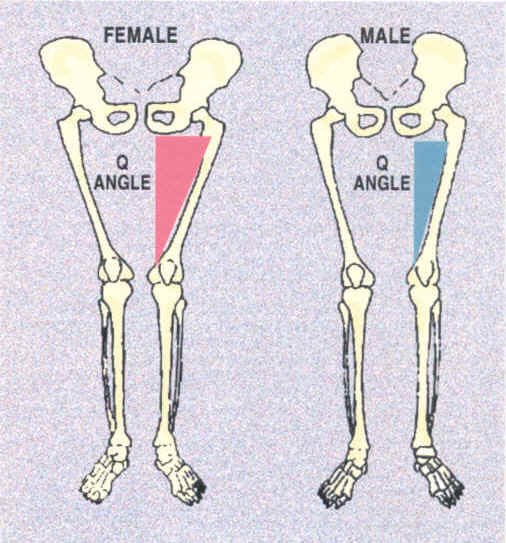
Females tend to have a higher Q-Angle due to wider hips. The research is murky whether or not higher Q-Angle leads to more injuries, but honestly I’m not concerned about that as much as the biomechanical relevance of a higher angle.
Females tend to have a higher Q-Angle due to wider hips. The research is murky whether or not higher Q-Angle leads to more injuries, but honestly I’m not concerned about that as much as the biomechanical relevance of a higher angle.
When hips are wider, the sacrum is in a relatively higher amount of counter-nutation and the pelvic bones follow it into:
- External rotation
- Abduction
- Flexion
- External rotation
- Abduction
- Flexion
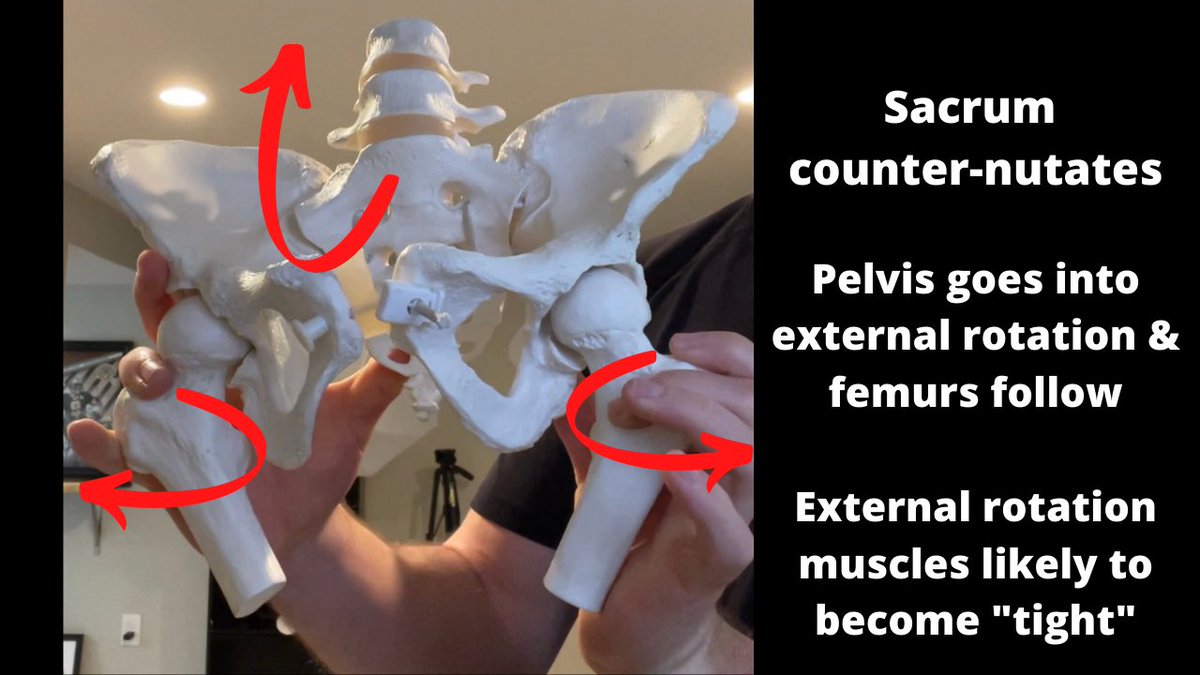
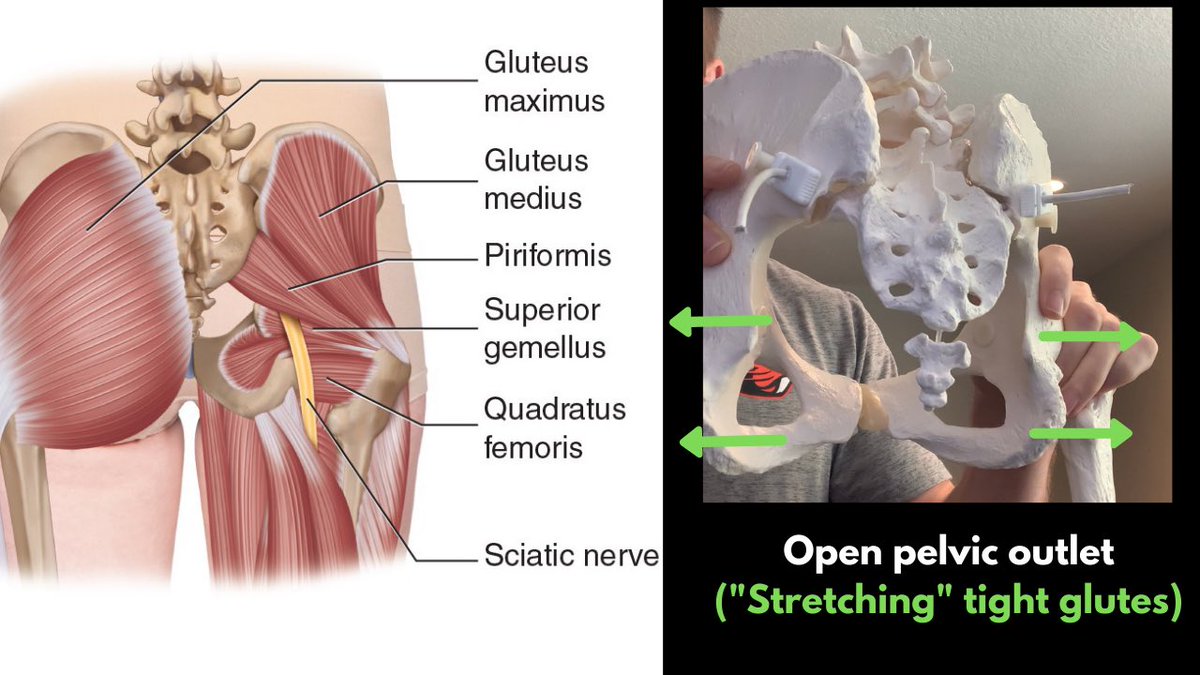
You can see how this could cause the deep hip external rotator (ER) muscles to become “shorter” or more “tight”, like the piriformis, glutes, and obturators.

Maclntyre et al, 2008 compared patellar mechanics between knees with no pain and with pain. They found the painful group had a statistically greater lateral shift of the patella, which happens often when Q-Angle is higher.

So if many females have a bias towards ER, why do they have weak ER muscles?
In my opinion it’s because muscles need to stretch to contract effectively. Just because muscle is “tight” does not at all mean it is strong.
What I often see is females
In my opinion it’s because muscles need to stretch to contract effectively. Just because muscle is “tight” does not at all mean it is strong.
What I often see is females

lacking strength in those muscles because they can’t effectively recruit them due to a lack of internal rotation (IR) capabilities of the pelvis and femurs.
There are a TON of theories why they are more predisposed ACL tears, but one aspect of it is related to a lack of hip IR.
There are a TON of theories why they are more predisposed ACL tears, but one aspect of it is related to a lack of hip IR.
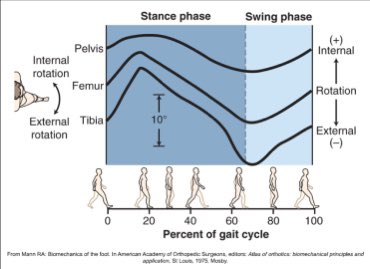
If the pelvis and femurs can’t find IR, the femur has a tendency to collapse inwards in an attempt to “find” that IR. Since the lower leg is biased towards ER, the tibia typically likes to stay in ER.
Femoral IR + Tibial ER = Knee valgus.
Femoral IR + Tibial ER = Knee valgus.

If there is concurrent femoral IR + Tibial IR + good pronation at the foot, this is normal and knees slightly coming inwards isn’t necessarily bad.
So a key to helping females stabilize knees would be to improve their IR. I have a thread on that here:
So a key to helping females stabilize knees would be to improve their IR. I have a thread on that here:
https://twitter.com/conor_harris_/status/1317219020299366401
This is just one possible explanation.
Other things that help reduce knee injury potential are:
- Increasing relative max strength
- Emphasizing training in three planes of motion
- Plyometrics programmed appropriately
- Adequate nutrition and sleep
Other things that help reduce knee injury potential are:
- Increasing relative max strength
- Emphasizing training in three planes of motion
- Plyometrics programmed appropriately
- Adequate nutrition and sleep
• • •
Missing some Tweet in this thread? You can try to
force a refresh