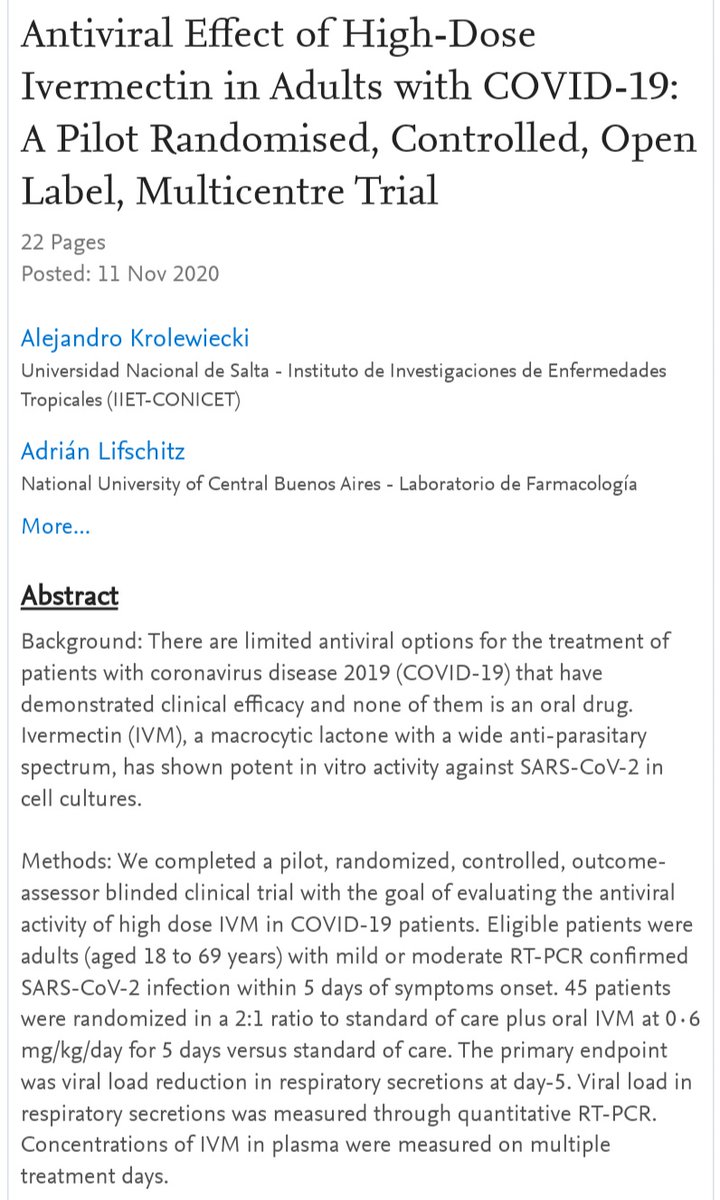
Recent RCT demonstrates reduced viral load in patients treated with ivermectin.
papers.ssrn.com/sol3/papers.cf…
Along with the post-exposure prophylaxis trials, this further indicates genuine antiviral activity in vivo for ivermectin (not merely anti-inflammatory).
papers.ssrn.com/sol3/papers.cf…
Along with the post-exposure prophylaxis trials, this further indicates genuine antiviral activity in vivo for ivermectin (not merely anti-inflammatory).
https://twitter.com/AOlavarria/status/1326623353717858306

See here for a few other relevant studies:
https://twitter.com/__ice9/status/1325018288997490689?s=19
The only study in vitro for ivermectin against SARS-CoV-2 used Vero cells and did not pre-treat at all.
This made it difficult to infer much about the effect during an ongoing repository infection in humans. Initial estimates looked unhittable.
https://twitter.com/__ice9/status/1324236638160146434?s=19
This made it difficult to infer much about the effect during an ongoing repository infection in humans. Initial estimates looked unhittable.
*"respiratory" typo
• • •
Missing some Tweet in this thread? You can try to
force a refresh