Excited to share our latest paper on bariatric surgery options, now out in @AnnalsofSurgery.
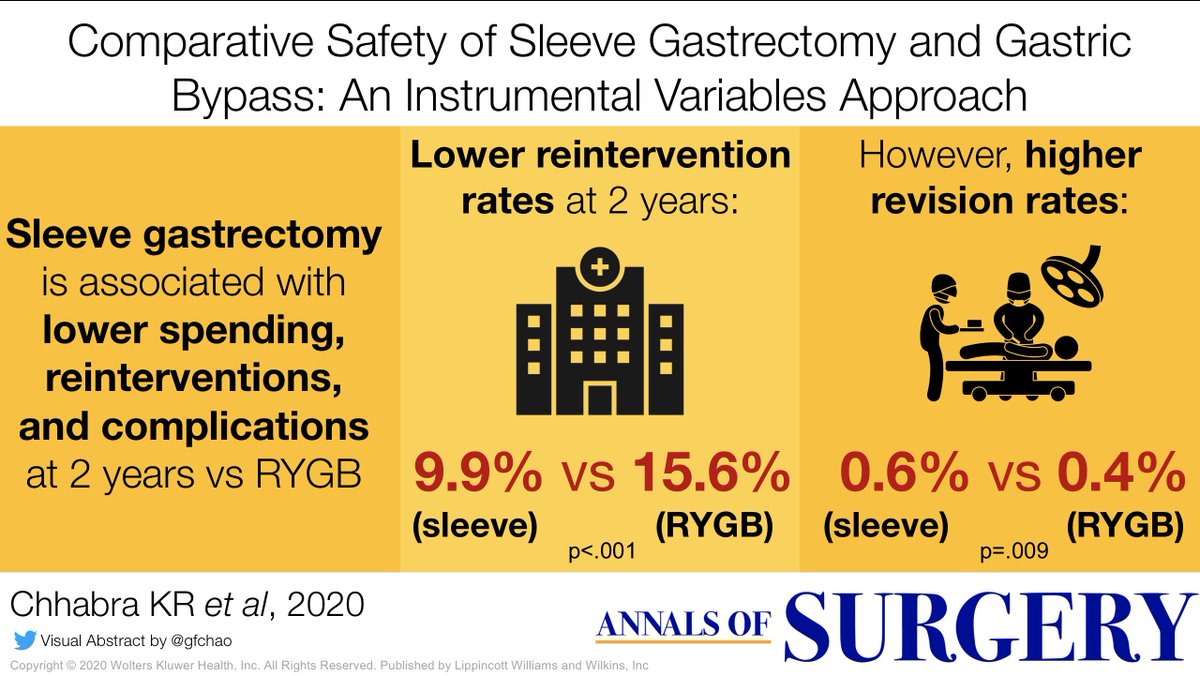
Sleeve gastrectomy is now the most popular bariatric operation, but RCTs of sleeve vs bypass are too small to tell us if sleeve has higher rates of rare complications (e.g. revisions).
Sleeve gastrectomy is now the most popular bariatric operation, but RCTs of sleeve vs bypass are too small to tell us if sleeve has higher rates of rare complications (e.g. revisions).
https://twitter.com/AnnalsofSurgery/status/1331227572256980996
Observational studies--on the other hand--are always subject to confounding. Healthier patients with lower rates of reflux are more likely to get a sleeve, so if bypass looks worse in observational studies it could be due to baseline differences.
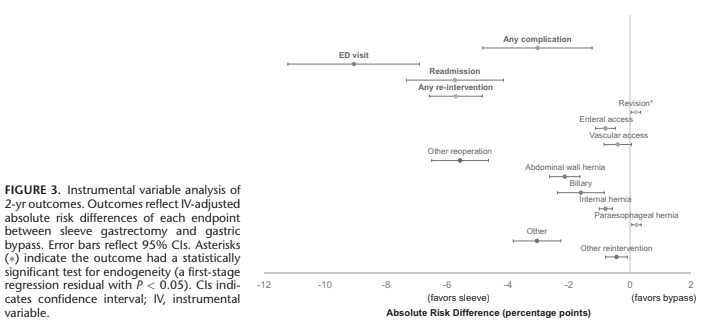
We looked at 38,153 patients who underwent sleeve or RYGB in the Marketscan commercial insurance claims database. We used instrumental variable methods to account for unmeasured confounding--exploiting state-specific variation in the year when sleeve took off as the IV.
We found that in both unadjusted & adjusted analyses, sleeve gastrectomy has lower overall rates of readmissions, complications, and re-interventions at 30 days and 2 years. Total healthcare spending was also lower w/ sleeve ($48K) than bypass ($55K) at 2 years.
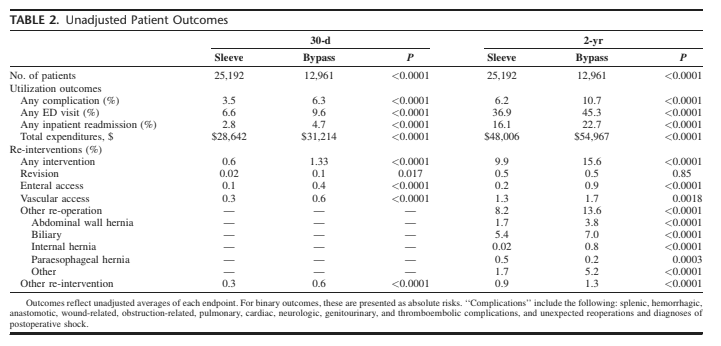
But in the IV-adjusted analysis, we found that sleeve gastrectomy actually had HIGHER rates of revisions at 2 years. We did NOT see this in the unadjusted or logistic regression-adjusted data. The difference was small (0.6% vs 0.4%) but statistically significant.
What does this mean?
Sleeve gastrectomy is overall safer and leads to lower healthcare spending than gastric bypass, even when you account for unmeasured confounding.
Sleeve gastrectomy is overall safer and leads to lower healthcare spending than gastric bypass, even when you account for unmeasured confounding.
BUT there are potentially important differences in revision rates, which may become bigger & more concerning as we look beyond the 2 year mark (which follow-up studies will do).
Finally: IV methods are useful outside econometrics, for measuring clinical outcomes where RCTs aren't feasible or powerful enough. In surgery there are MANY situations when an RCT is not practical or possible--but there are other ways to figure out what's best for patients.
Appreciate all the colleagues & mentors who made this study possible: @gfchao @DanaTelem @davearterburn @Andy_Ryan_dydx J Yang J Thumma B Blumenthal @jdimick1, @UMichCHOPFellow & @ncspMICHIGAN for support, & @AnnalsofSurgery for publishing!
• • •
Missing some Tweet in this thread? You can try to
force a refresh