,
9 tweets,
6 min read
Read on Twitter
THREAD:
Our study on Medicare readmissions penalties for surgical patients is now out @Health_Affairs
.healthaffairs.org/doi/full/10.13…
We found that the pace of readmissions reductions in joint replacement *decreased* after targeted penalties were announced. Sound strange? Read on.
Our study on Medicare readmissions penalties for surgical patients is now out @Health_Affairs
.healthaffairs.org/doi/full/10.13…
We found that the pace of readmissions reductions in joint replacement *decreased* after targeted penalties were announced. Sound strange? Read on.


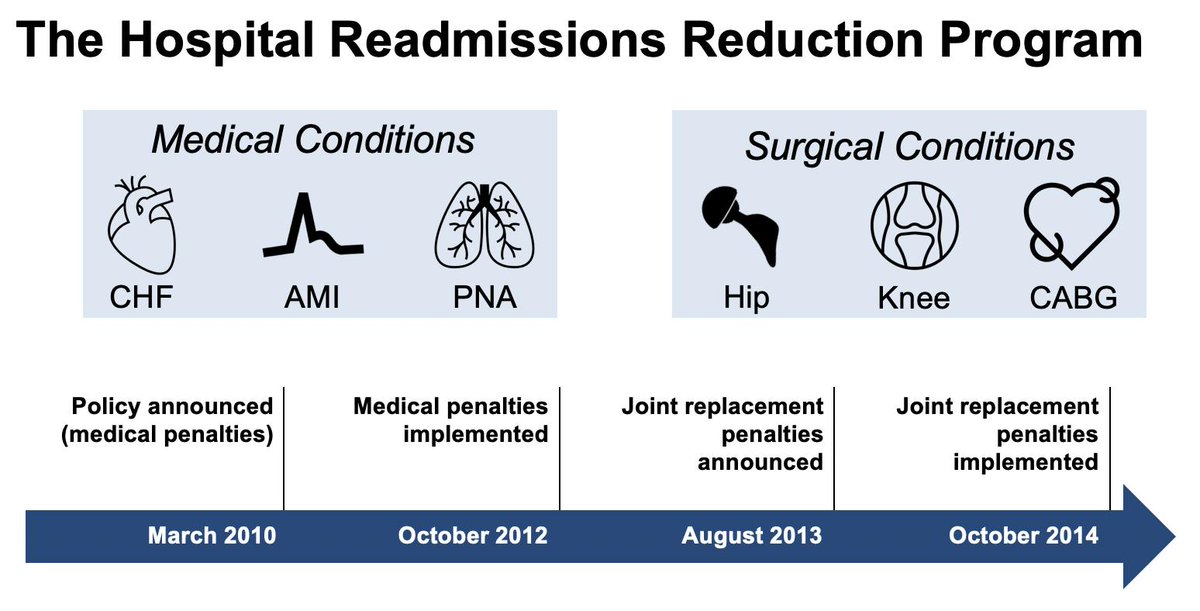
Medicare started penalizing hospitals with high readmissions rates for 3 medical conditions way back in 2010. In 2013, they added hip and knee replacement patients to this program. And they have continued adding more conditions since then.
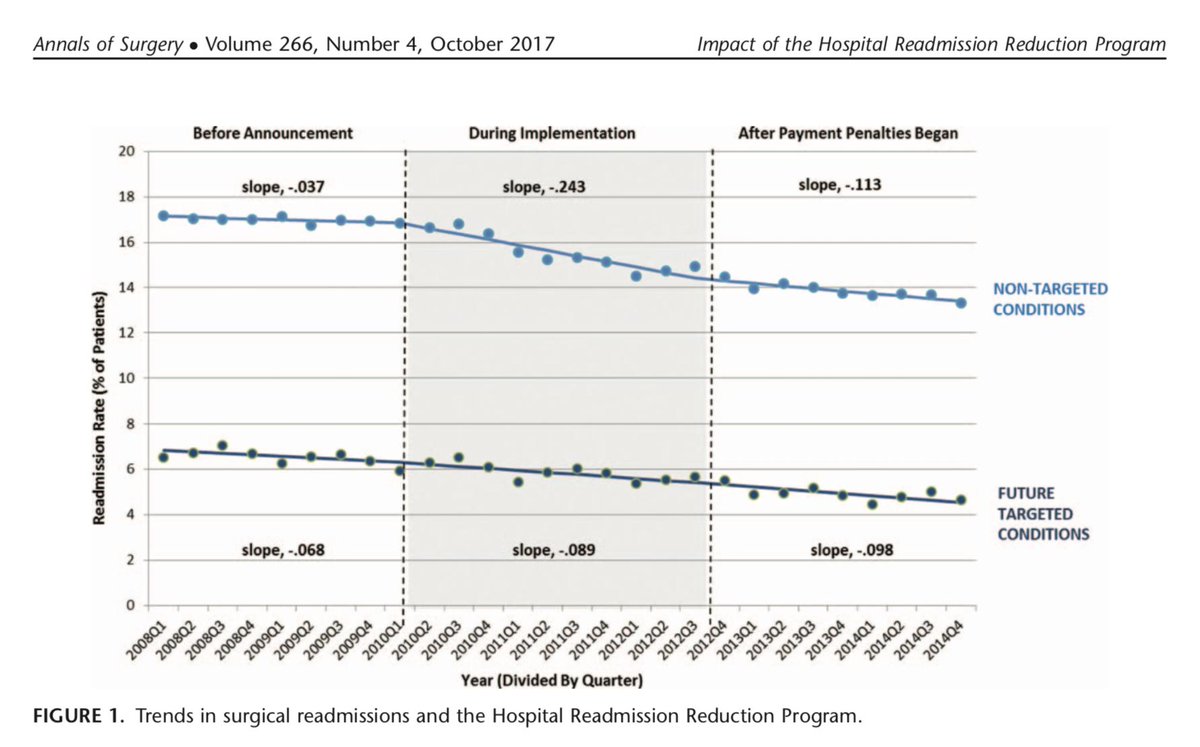
After medical penalties came out, medical readmissions dropped quickly. But so did surgical readmissions: journals.lww.com/annalsofsurger…
What's unclear is whether announcing surgical readmissions penalties led to any additional improvement.
What's unclear is whether announcing surgical readmissions penalties led to any additional improvement.
We're also starting to see that the program was not as helpful in medical patients as we once thought. Changes in Medicare billing led to artificial increases in comorbidities, which led many studies to overestimate the program's impact.
jamanetwork.com/journals/jamai…
jamanetwork.com/journals/jamai…
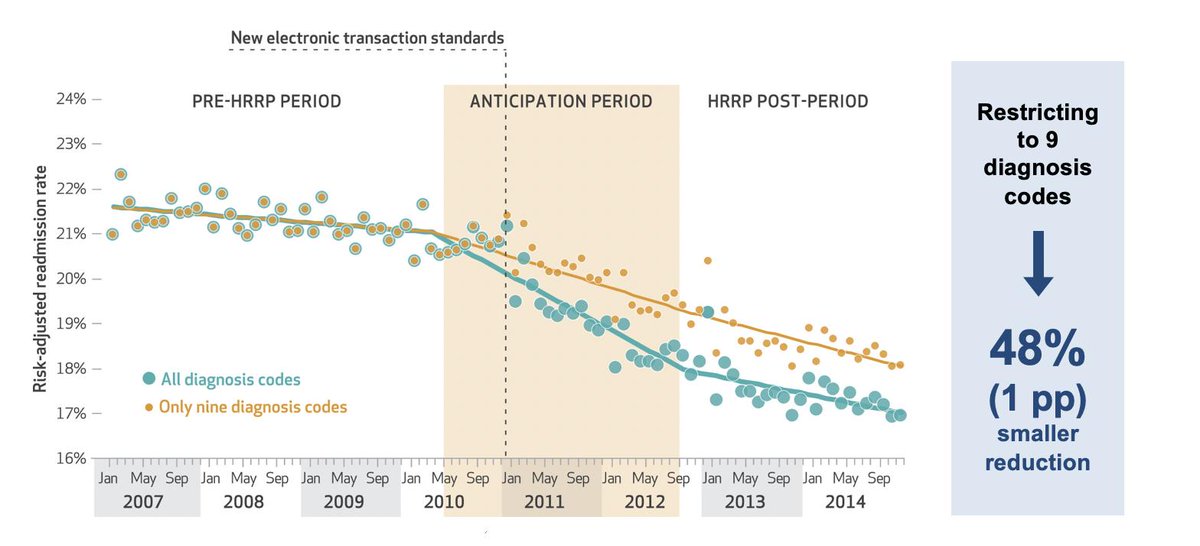


Using Medicare claims for hip & knee replacement, we find that surgical readmissions were decreasing before 2010, then decreased *faster* after medical penalties were announced. But these decreases *slowed* to baseline after surgical penalties were announced in 2013.

To gauge the effect of upcoding, we removed comorbidity adjustment from our models, and didn't see much change in this pattern. The change was -2.1 percentage points with risk adjustment, or -1.7% without risk adjustment.

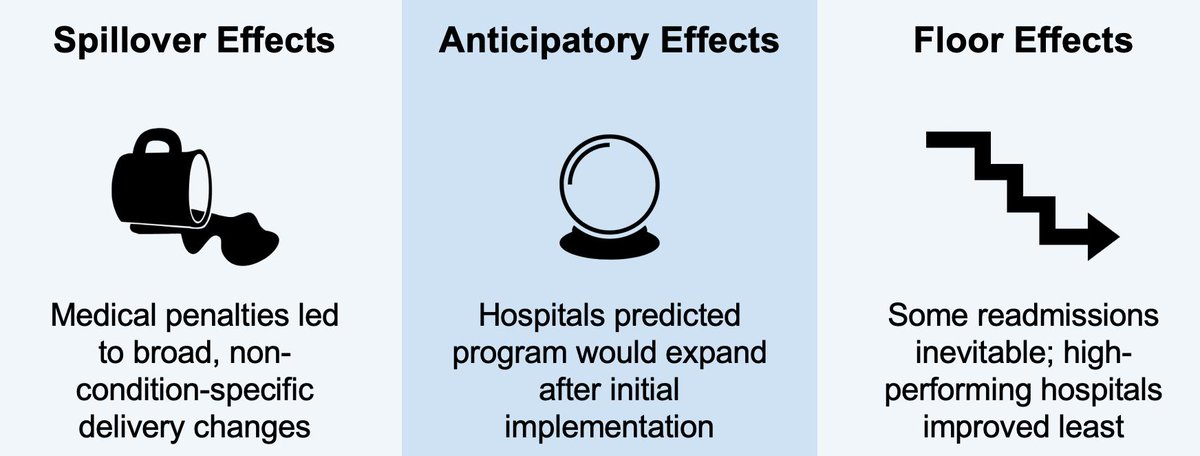
Why didn't surgical penalties work? 3 ideas:
#1, the penalties led hospitals to make "spillover" changes beyond the targeted conditions
#2, hospitals anticipated that surgical penalties were on the way
#3, when surgical penalties hit, there was no more room for improvement
#1, the penalties led hospitals to make "spillover" changes beyond the targeted conditions
#2, hospitals anticipated that surgical penalties were on the way
#3, when surgical penalties hit, there was no more room for improvement
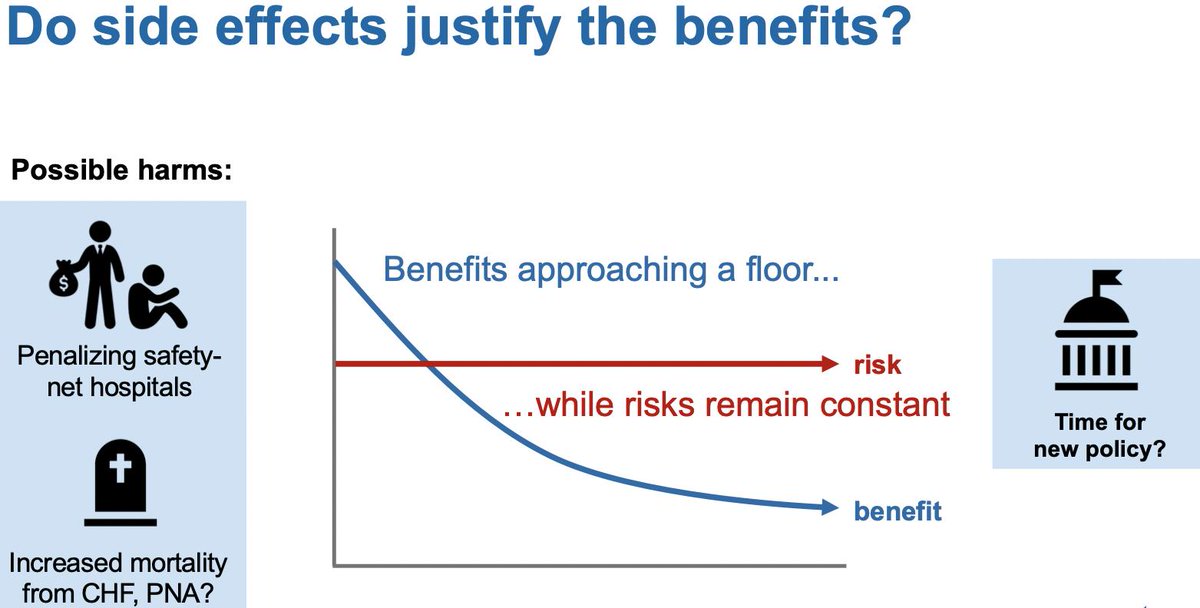
Which begs the Q, why are we expanding this program at all?
There may not be much juice left to squeeze out of readmissions. Hospitals may be doing bad things to avoid penalties (like sending patients home who actually need an admission). Risks may be overtaking the benefits.
There may not be much juice left to squeeze out of readmissions. Hospitals may be doing bad things to avoid penalties (like sending patients home who actually need an admission). Risks may be overtaking the benefits.
Would welcome feedback: healthaffairs.org/doi/full/10.13…
DM me if you don't have access.
Grateful to my coauthors @AndrewMIbrahim, Jyothi Thumma, @Andy_Ryan_dydx @jdimick1 at @UM_IHPI; @AcademyHealth for opportunity to present, & @Health_Affairs for publishing.
FIN
DM me if you don't have access.
Grateful to my coauthors @AndrewMIbrahim, Jyothi Thumma, @Andy_Ryan_dydx @jdimick1 at @UM_IHPI; @AcademyHealth for opportunity to present, & @Health_Affairs for publishing.
FIN